Some decades ago, there was a weekly column in The Spectator. When the inebriated columnist, gripped in his local Victorian London pub by a hepatic illness of his own making was unable to write, in lieu of the absent column appeared his doctor’s sick-note: JEFFREY BERNARD IS UNWELL.
SO IS TCP. Most especially after reading the excellent, on-point but extremely depressing histopathological autopsy cases in, VACCINATED – DEAD.
Unlike Mr Bernard, the self-cure for TCP is an expurgating dose of book review, and not like Jeffrey, tumbling back into Soho after a few.
This slim, but densely factual and telling atlas of cases is the most damning indictment of covid jabs’ killing powers. It is written in translation from the original German by colleagues of the Late Professor Arne Burkhardt. He was a pathologist who came out of retirement to discern the pathological truth of the numerous deaths happening in shocking synchronicity and too close in time and space to the purported lifesaving covid jabs.
The continuing, systematised whitewashing, suppression and concealing of the immediately-apparent, gruesome truth of the fast-tracked jabs remains more shocking.
The book is the very information I and like-minded physicians needed in 2021 to confirm and encourage further disclosure of what we already thought we knew, until the government made with multiple sophisticated menaces and misinformations the opposite to be believed.
Instead, the devils of the mafia-enabling MHRA, Ofcom, GMC and the propaganda machine formerly known as journalism conspired with our public health officials against public health. The world has forgotten the woman who steered the General Medical Council during covid on a suicide course to destroy medicine was former paediatrician and GMC Chair, the Late Dame Clare Marx.
She stepped down in July 2021 following a diagnosis of pancreatic cancer, finally dying in late November 2022. She would have been at least double-jabbed, by then. It would verily be supreme tragic irony if she in fact succumbed to SV40 and DNA contaminated COVID-19 ‘vaccines’ via any of the 13 carcinogenic mechanisms proposed by Professor Angus Dalgleish. Yet, her successor and her organisation continue, as headless chickens unable or unwilling to gain proper perspective of the crime they, at once, are part of and which they part oversee.
Many Germanic Heroes
Professor Lang and Ute Kruger should be guests on every source and form of mainstream and social media decrying the crime. The reality is closer to the new normal: no one knows, no one cares, and the covid measures mass democide is overshadowed by the same actors creating multiple theatre wars and an ethnic-cleansing by genocide for their continuing pecuniary gain.
The book is sombre and sobering reading. In particular for one who has witnessed the sordid unfolding of this massive medical lie within thousands of patient consultations over five years.
It is a definitive handbook for the histopathological causes of the in vivo, realtime pathology one witnessed in ones’ poor, preternaturally terrified, but hopeful patients. Those who queued for miles around the corner for their lives to be saved by the medical and nursing professions. How many queued for their premature and predictable deaths?
This scientific analysis makes one think even more died than the extraordinary mass killing one had already apprehended and foresaw.
To see the case reports of these poor, dead and often young humans alongside the photographs of their histological tissue samples contextualised by the clear relationship in time, space and pathological mechanism to covid jabs makes for a profoundly distressing read.
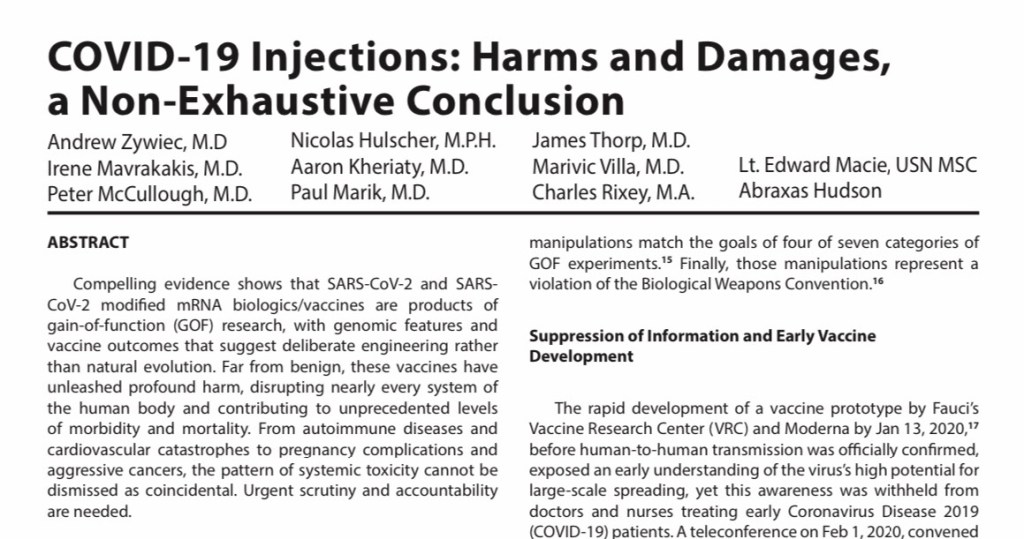
The basic method, as with the most graceful medical and scientific proofs is, on the face, simple. Immunochemical staining of the damaged tissues with spike protein but not nucleocapsid protein is reasonably presumed to be damage by injected, pharmaceutical modified mRNA, and not by the elusive SARS-COV-2 purported to be the product of US funded gain-of-function bioweapon research.
The consistent presence of the unusual so-called ‘white clots’ reported by embalmers everywhere, resonates with the coagulated masses of blood-pauce fibrin found by this team. Amyloid-like deposits – about which I have written of as a possible cause of an emerging neuropsychiatric pandemic – and unexpected, dark inorganic, carbonaceous crystalline matter deeply sequestered in multiple human organs of the same cadavers abound as indelible evidences of a very peculiar, multiple homicide international crime scene.
The dark organic matter is notable, for the good pathologists leaving it there. However, anyone in the know realises the inference: injectable graphene derivatives and nanotechnology. Once one has evaded or waded through the swamp of misinformation laid by Google, one easily sees graphene oxide is an object of pharmaceutical interest for its cytotoxic and inflammatory effects.
Indeed, if it is pro-inflammatory (it is), it is an experimental candidate for a vaccine adjuvant. See this 2016 lecture on Cellular Responses to Graphene Oxide Sheets by Dr Sandra Vranic at CLINAM (European Foundation for Clinical Nanomedicine), Basel.
The bluetooth coupling, magnetic deltoids do not seem so conspiratorial, now. Particularly, in light of the numerous patents and university departments outlining such things. We now know for sure that graphene oxide has been discussed as a vaccine excipient precisely for its pro-inflammatory nature.
One recalls the German scientist Dr Andreas Noack (who claimed his PhD included the conversion of graphene oxide into graphene hydroxide). This man was an expert in graphene and its derivatives, and his righteous indignation at the covid jab crime led to a live-streamed raid by armed German police upon his home. Sometime later he suffered an untimely death in the arms of his pregnant wife. It was convenient for only those wishing to suppress the man’s expert truths.
Germans not only figure prominently in the State implementation of covid-related mass denials of liberties and bodily autonomy, but also in their fine antagonists. Think of Drs Wolfgang Wodarg, Sucharit Bhakdi, Heiko Schöning, Reiner Fuellmich, and Michael Palmer. Nearby, across the Alps was Swiss cardiologist, Dr Thomas Binder, preposterously detained under the mental heath act for pointing out the obvious concerns of the covid narrative. All at some point were ostracised, arrested, charged and/or jailed, and one even labelled the most specious of curses, anti-semite.
Dr Thomas Jendges, a leading German doctor became a casualty of the covid era after he fell from his hospital rooftop in an alleged suicide. Despite Reuters best attempts to debunk this by loosely associating one wild report with other more based reports, Lord Mayor Sven Schulze said on the morning of 2.11.2021:
“It was with great dismay that I had just learned of the tragic death of Dr. Thomas Jendges, the managing director of our hospital. Just last night we exchanged ideas for a long time about the difficult corona situation.”
He just happened to leap off the hospital rooftop a few hours later. Doctors do this all the time. Move on. Nothing to see here? Dr Rose furnished us with more, as did Stess News, and Las Republicas.
In recent German elections, 16 candidates, including 7 AfD members died just before polling. Dr Fuellmich was politically active in Germany with die Basis. He was a powerful and eloquent counter voice until he was detained in Mexico and extradited to Germany. The detention increasingly looks not only like injustice but a deliberate State attempt to silence him by politically imprisonment. It has worked. He has a successful record of bring fascist corporations to heel and legal account. No doubt he would have done the same to Pfizer and Co. All chance?
Further clinical coincidences come thick and fast reading Vaccinated – Dead.
Vaccinated – Dead documents a pandemic of clinicians overlooking the obvious temporal correlation of covid jabbing with acute and chronic morbidity and mortality. Then, a laundering of that with nonchalant primary autopsy diagnoses in silenced, jabbed corpses, each inexplicably riddled with unusual, co-existing, multiple pathologies.
Suspicious, bereaved families sought secondary histopathological examinations. These uncovered physical evidence of multiple, strange, and sometimes novel findings entwined in a murderous noose of amyloid-like, fibrin, and black, crystalloid, carbonaceous deposits. Threads sodden with liberal doses of multi-system lymphocytic infiltrates, all immunohistochemically linked to covid jabs.
How my own extraordinary clinical observations as a lowly, lonely clinician somewhere off the continent can so closely mirror my German laboratory colleagues’ is (to paraphrase Fleming) not mere happenstance, and not even coincidence, it implies enemy action.
Casebook Examples
Cardiovascular pathology
Take, for instance, my young female patient with a very rare case of post-covid injection aortitis in 2022.
There are several aortitis cases and many cases of cardiovascular system inflammation and thromboembolic disease in this book. They ably provide convincing pathological bases of modified mRNA injectables driving disease and death.
Take, for example:
Case 10, page 79, dead 61y male: aortitis, aortic dissection with wall rupture, pericardial tamponade, massive vasculitis prostatitis. I recall vividly my friend’s relative, a mid 40s male inexplicable developing acute urinary retention a week or so after his first covid jab in early 2021;
Case 66, page 35, died suddenly on a park bench after surfing, 48y male: aortitis, pericarditis, thickened pericardium with amyloid-like characteristics, myocarditis with loose interstitial scarring & amyloid-like characteristics;
Case 17, page 24 & 25, dead 83y female: multiple myocardial black, crystalline deposits of uncertain origin, some needle-like, often with corkscrew-like ends;
See:
My patient and a doctor discussing their multiple clots in November 2021.
Three siblings near-simultaneously falling ill, two victim to serious cardiovascular events in December 2022.
Dermatological pathology (with Clots, Vasculitis and Hypertension)
Case 39B, page 22, 127 & 128, 43y female: blood sample containing homogeneous, non-layered fibrin thrombus… vascular changes are well compatible with the clinical finding of increased peripheral resistance in the capillary bed [ie a risk factor for hypertension]… amyloid deposits in the vessel walls… perivascular lymphocytic vasculitis… significant proliferation of dendritic cells in the epidermis;
Case 113B, page 29 &129, 38y male: cough, pleuritic chest pain, headache, brain fog; significant rarefaction of basement membrane elastic fibres… disruption and fragmentation of elastic fibres within the deeper dermis;
I refer you to:
The general rising pathology and inexplicable severe hypertension cases I reported in 2022.
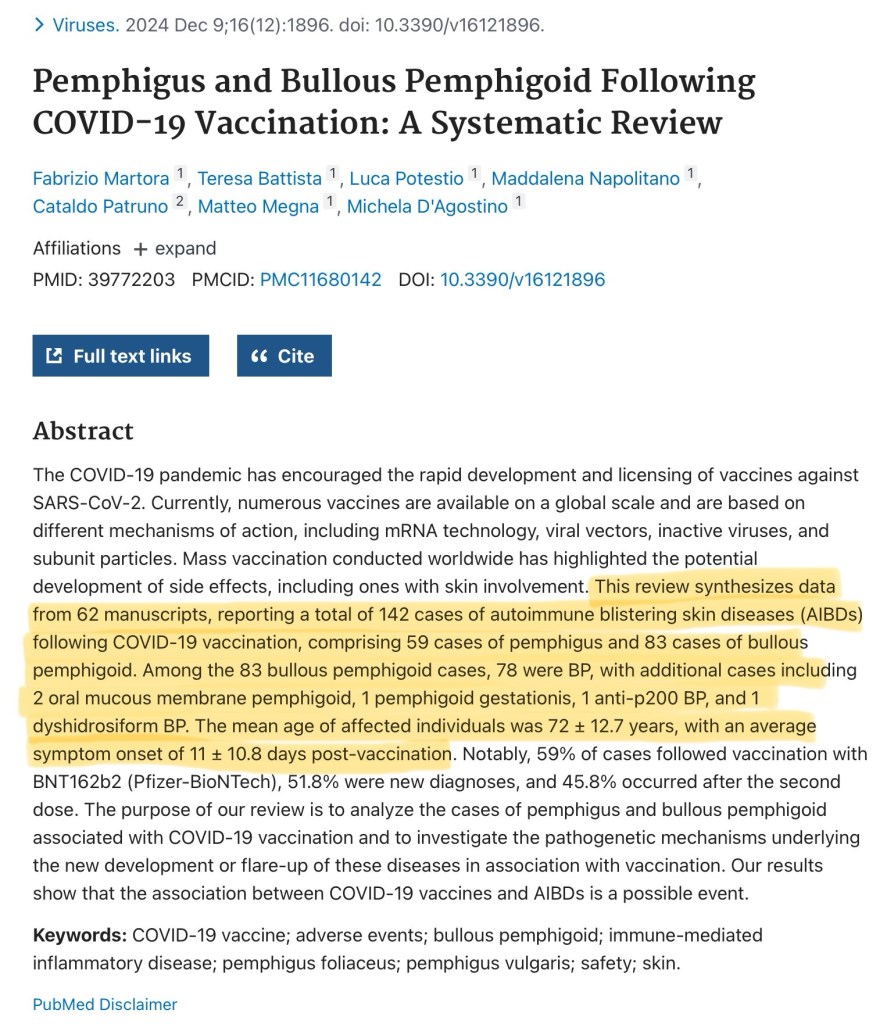
The series of pemphigus and pemphigoid rash patterns in my patients, post-covid jab.
Case 42, page 94, dead 84y female: admitted for shingles following her 1st jab, only to be opportunistically diagnosed with asymptomatic covid in the hospital; she was most likely given a ‘curative’ second jab by the hospital, only to die 17-33 days after discharge;
Case 42 typifies the murderous pandemic of State-sponsored wrong-thinking and wrongdoing which is increasingly occurring all over the Western world. See my 88y patient with recurrent post-jab shingles in November 2021.
Neurological pathology
Case 60, page 53, dead 72y female: brain haemorrhages, inflammatory changes, infarction with partially dilated blood filled vessels with surrounding lymphocytic infiltrate, patchy fresh haemorrhages. Amyloid-like hyaline material in the brain blood vessel walls;
Case 120B, page 129, 63y female, presented with hemiparesis, ataxia, character change: encephalitis, brain vasculitis, amyloid-like brain deposits, lymphocytic & phagocytic infiltrates;
I have written in detail regarding my clinical experience and emerging suggesting covid jabs are associated with increasing prevalence and prematurity of chronic neurological illness and cognitive impairment in March 2025.
Gonadal pathology (with Myocarditis and Clots)
Case 18, page 66, dead 29y male: disorder of spermatogenesis,
Case 56, page 65, dead 85y male: lymphocytic testicular inflammation;
Case 157A, page 132, 15/40 abortion material (after intra-uterine death): both father and mother triple vaccinated; Gravida 5, Para 1 mother gave birth in 2018, but subsequent 4 unsuccessful pregnancies inter- and post-covid jabs. Spike protein positive, nucleocapsid negative endometrium;
Case 159, page 31, dead 16y female: myocarditis, subclavian and brachial vein thrombosis, spike protein detected in ovaries;
Here, we have explanations for menstrual disturbances, and miscarriages I noted were occurring uncommonly frequently, and a validation of the officially ignored, logical infertility concerns raised by Drs Wodarg and Yeadon on page 5 of their December 2020 petition, about which I commented, here, also in 2020.
See:
My 36y female patient of November 2021 with post-jab dysfunctional uterine bleeding;
and, my 40y female patient of November 2021 with post-jab secondary amenorrhoea since the second jab.
In fact, I wrote to various government officials in July 2021 warning them that many of the above realised ADRs and disease were occurring, and were highly likely to occur, according to the evidence of that time. In May 2023 I added further concerns regarding post-covid jab related emergent disease patterns.
As with other studies and other clinicians’ reported experiences, my clinical experience corroborates well with the findings of Prof Burkhardt’s team. Experiential evidence of this clinical sort is compelling but continually attacked and ignored. The many post-covid jab deaths were hidden and not flagged by the medical and coronial systems. These deaths were mass-misattributed and fast-tracked to cemeteries by purposely degraded medical and death-certification systems.
Transthyretin Amyloidosis
Tafamidis, is being pushed under the brand name Vyndaqel by Pfizer for the treatment of transthyretin amyloidosis with cardiomyopathy. This month, I happened to attend a lecture with a Pfizer drug representative advertisement force-fed into the middle if it. The FDA is said to have approved this use in May 2019. This type of amyloid is implicated in multi-system disease and is now being implicated in covid jab pathology. Is this another supreme irony, where Pharma take with both hands, Pfizer jab cardiomyopathy, etc, followed by Pfizer Vyndaqel?
Medical Risk
Prince Monolulu & The Diamond Princess
Vaccinated – Dead is sobering for other reasons. Reading it, one contemplates upon those of my colleagues who were well-meaning but ignorant and propagandised, and their hapless patients.
One thinks of the normalised, inherent danger of old normal medicine. How simple routine procedures can unexpectedly and suddenly bite back, taking the life of a fellow, dear human patient rapidly away to somewhere on an autopsy gurney. The cost of failure is truly dear.
It is painful, because it, once, happened to TCP. No matter what one’s noble intent, no matter the desire to do one’s best for one’s patient, sometimes even in the safest of health systems, it does go catastrophically wrong. One is caught in the eye of a storm in deathly embrace with a patient. One mourns the death more deeply than one’s own blood. It is usually less common than what occurred with global, centrally-cascaded covid measures.
Life is an inherently risky business. Even offering a friend a sweet can be fatal, as Jeffrey Bernard discovered when he offered his unwell, good friend, Prince Monolulu a strawberry cream chocolate. Whilst, sat beside the hospital cot, he wished him better health. This fraternal action turned the cot immediately into his now choking friend’s deathbed. Presumably, there was no intent to kill in this ritual act of brotherly nourishment, proffered from a deadly box of ironic Black Magic chocolates.
Dealing in the voodoo of medical cures often carries the heaviest risk of death, as this doctor learned at a heavy, lifelong cost. We are forever on the cusp of ending a life on the end of a needle or the nib of a penned prescription for oral penicillin. Even the most successful scalpel can end down the road in sepsis and premature, unexpected death.
How many has one killed but not even realised?
However, covid has ushered in a new era of carelessness so reckless it is tantamount to intent, negligence so bad it is manslaughter. The act of the State-suppressing knowledge that covid jabs were so seriously harmful is so bad that government officials’ actions and inactions are complicities in mass medical murder.
Most disturbingly of all, in spite of all the facts, this poisonous mixture continues to be purveyed to selected vulnerable individuals. It is as if those who commit the crime hide it by attempting a slow, imperceptible retreat, killing as they slither away.
It is said each doctor has a cemetery of dead patients within his heart. Those deep ventricles are a Davy Jones locker full of dark secrets and trauma. The agonising calculus of squeezing maximum benefit for no harm has always proven to be impossible. No matter how hard one tries to do good, very bad things, on occasion, happen.
Only if one has ever been in that wretched position, will one understand. One is left with a patient dead body and one’s own stripped of its soul. Hero Complex, at once, becomes Absolute Zero Complex.
One might wake at midnight and see the dead patient’s death in one’s eyes, or in the bleary eyes of a mirror, toothbrush in mouth. In one’s dreams, on the street, in the supermarket. One sees it in the eyes of every patient who smiles, takes ones hand and gives thanks for one being the greatest, kindest doctor ever, the only one whoever listened and helped. If only they knew. It remains forever unbearable.
There are some special medical environments where we might further forgive noble but fatal errors of judgement and genuine, unavoidable complications. Those environments are typically in theatres of war, or in impoverished countries where there is chaos, poor system and little resource.
What remains unforgivable is the meticulous method with which chaos, poor system and little resource was wilfully created and imposed in the West. All for a common cold, which was proven very early on in the faux pandemic propaganda to be just that by the Diamond Princess study.
Even those professionally trained to kill are forever changed and traumatised by it. Somehow, the systematic, mass killers are immune to the grief of it.
Officials such as Matt Hancock and Antony Fauci must have cemeteries of hundreds of thousands of bodies trapped inside their blotted chests. The deep guilt of having one body’s blood inadvertently on one’s hands is intolerable; how much more might theirs be? How much more atonement and redemption for their sins? Why do their hearts not also burst with the pain?
Conclusion
This book, necessarily written in adversity with risk to its team, is truly an extraordinarily calm, and scientific exercise in medical understatement. It is an utter damnation of modified mRNA gene therapy. It offers chilling, woefully unique and rare insight into a global crime scene. No wonder it is ignored by those who profit from it. Those who are extremely powerful and wield an increasingly centralised digital wand which imposes tyranny, mesmerises masses and manipulates reality. We are persuasively killed by State cures and soothed by the salve of State lies. This little red book is the indelible evidence of their multiple homicides.
It is because of Prof, Burkhardt and his team’s courageous scholarship these poor slaughtered souls have been given powerful voices from beyond their premature graves.
This book is a stained histopathological, photographic history of the stinking truth of the covid crime and it deserves so much more attention and accolade. It should be mandatory reading for all doctors. It a quiet, reserved but shining exposé. The likelihood is it is already victim to an internet misinformation vortex viciously vacuuming truth, reason and morality from our world.
Buy a copy and lend it to your misinformed doctors, this Christmas.
28th November 2025
Please let me know in the comments about your own, related experiences. Please share this with your doctor, and let me know the response.
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, on web.archive.org
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, as prescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
Dr. TCP tweets at @tcp_dr, Blogs here & Substacks here.
To support TCP please share and retweet.