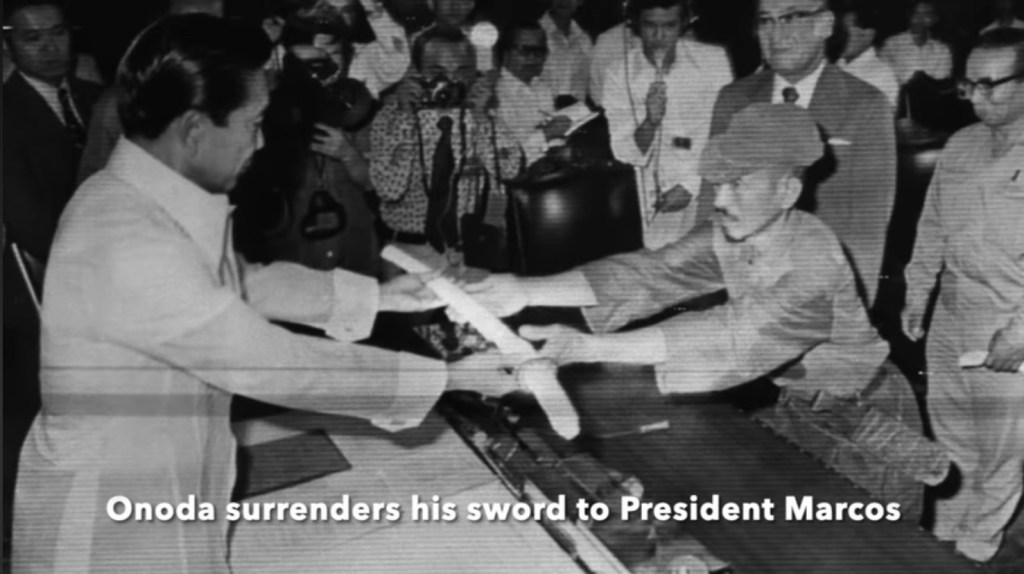
Perennially Entrenched: 2nd Lieutenant Hiroo Onoda surrendered in 1974, an astounding 29 years after the end of WWII
Another interim despatch from the mundane, microcosmic, rump end of COVID-19: The Greatest Show On Earth. It indicates that potential adverse effects of the current rounds of JCVI and government-recommended covid jabs continue to be felt in our communities and go unacknowledged by our authorities and the mainstream. It continues to prove that as sure as sheep are sheep, so are most of us.
I continue living covid, still livid at covid: the jabs, a ritual mass poisoning. Long after VIC, Victory in Covid Day went at once unannounced, presumed, denied and claimed. All whilst covid (the pandemic bit) never happened. The conspiracy of jabs for profit and control remains hard to criminally prove, and the admission of damage and guilt politically unacceptable. These competing narratives remain lingering around me, after former colleagues have fled the profession prematurely, moved on in denial, or sold their souls more deeply.
This August was the 80th anniversary of VJ-Day, Victory Over Japan. The majority of Japan’s armed forces surrendered on 15th August 1945, but many small groups and individuals did not. Incredibly, the last recorded Japanese only surrendered in 1974, a mere 29 years after the end of WWII. Such entrenched behaviour reminds of the many colleagues and patients still bunkered down, in late summer 2025:
A late-summer flurry of positive tests, 2025
Mrs Banzai!
Autoimmune 55 year woman on an injectable immunosuppressant for a rheumatological condition, presenting with a very sore throat and temperature. Just tested positive for COVID-19 in the month August 2025. True to form, as an identikit child of peak commie-fascism, her priority is an ‘antiviral’ i.e. PaxlovidTM, or potentially even some kind of intravenous concoction of immunoglobulin.
These existential questions continue cropping up. Had she not tested positive, she would have perhaps remembered her priority was my priority: check the white cell count. The real threat was potential neutropenic bacterial tonsillitis. The real action: stop the methotrexate, start antibiotics.
Unfortunately, her five-year prevailing view was, ‘I will die of covid,’ because she is one of the patients who is made to feel perpetually clinical extremely vulnerable by the scriptwriters in Whitehall. Had she not tested positive for covid, I am sure she would not have thought, ‘I have flu, I need an antiviral, lest I die.’
Such cod narrative makes the doctor clinically extremely vulnerable, too. Fortunately, the digital formulary would not even give me the option of prescribing PaxlovidTM, and so I very gladly packed her off to A&E for someone else to do the damage to her, if she so wanted it. Before doing so, I explained that her condition’s priority, in my opinion, was not an antiviral. It never has been with most so-called viral infections. Covid has transformed the narrative. Patients and doctors now believe that just as antibiotic is to bacteria, antiviral maybe to virus.
Master Kamikaze-Parent, 17
Teenager with psychological issues. Actually, issues I suspect caused by Covid lockdown policy in school, and certain parental proclivities.
The parent wants antivirals for the son, for he has gluten intolerance which in the parent’s artificial intelligence-groomed mind means he has an autoimmune condition. To her, in turn, this means he is clinically extremely vulnerable. It is gobsmacking.
The family all have mere colds, and all test covid-positive. This, the parent uses as a reasonable argument against false-positives. I slip into her narrative. I beg to counter with the fact the original pandemic wasn’t at all dangerous to most, particularly not to children. Further, the government had conceded the pandemic was long over and therefore did not need to be associated with mass panic. It had reassured us the ‘variants’ were now even less serious than they actually were in the first place.
The paradox of her continued pandemic fear in 2025 despite the whole family being covid jabbed remains an unmentionable. This is the banality of abnormal health within the political incantation of the new normal. Again, I shield behind my inability to prescribe what the parent thinks the child needs. So it’s, listen to me or go to A&E. Listening to me wins, but, I believe, only because the hospital is too far away.
I would suggest the fact the family is all jabbed is exactly why it is all unseasonably feverish with a flu-like illness in the hot summer of 2025. The mother of that then 14-year-old child took her to have her two or three covid jabs – she can’t quite remember how many, just as she can’t quite make a link between them and their current malady.
Ms Chesty Cough, 55. A breath of fresh air.
Finally, that day, a middle-aged lady. Just returned from abroad, never jabbed, has done a covid test. It returned positive. With baited breath and trepidation I called her – what would such an clinical non sequitur possibly want? What she did want ought to be the final pragmatic epitaph to COVID-19: ‘Doctor, just returned from abroad, never jabbed, developed a chest cough and did a covid test which returned positive, just want some antibiotics, please.’ That it was not PaxlovidTM warmed my heart.
1974: Onoda surrenders his Pfizer to President Marcos
The Spring-Summer 2025 Covid Collection
The UK spring 2025 covid-jab campaign had presented its own particular revival of post-jab disease. The patterns are temporal, and so similar in clinical presentation as to, again, strongly imply not only a correlation but a causation. I submit yellow cards, I record my concerns, and I insert concern where I can when the patient is not too demented or liable to take offence (with a “what do you think this pattern might be telling you?”) and then I try move on, unflustered.
It is early May 2025, and we are at the end of about round 10 of the covid boosters. That thing which was only needed twice, safe, effective and that was all, the scamdemic having allegedly finally finished in summer 2022. Spring 2025 augurs another unseasonable wave of chest infections, hospital admissions, and frivolous hospital antiviral prescriptions. Add to that the new normal of weird covid jab-related pathology. Most seem to be in their seventies or over, and therefore prime, continued targets for their governments. Does it represent the cumulative burden of trusting obedience?
My consultation room has become a confession chamber for those elders:
Never, again, I am fed up.
Doctor, why are they still doing it?
More pertinently, why did you, and why do many of you continue to accept them?
Some geriatrics remain the obedient serfs of the landed gentry. No amount of capitalist hyper-individualisation and indoctrinated hyper-sexualisation with the freedom to copulate like juveniles on cruise liners in the Mediterranean has taught them to think critically, have faith or to self-respect.
Mr Barnacle Biceps, Late septuagenarian
Possible skin carcinoma, clinging like a large, ancient ocean barnacle to his lateral biceps, surrounded by hyper-melanotic macules. He says it only started soon after he had the initial covid jab in the exact site of its injection. He says it pointedly and with, I feel, an inappropriate relish, tapping at it, ‘EGGx-actly There, Doctor.’ He thought it would detach when bored and leap back overboard. It did not. For 4 years it has carried on growing, and growing. He is referred to the skin cancer clinic.
Intrigued, I follow the case like a limpet. The additional irony of it is he is seen by a distant plastic surgeon, online via a grainy, rural internet connection. My virtual colleague does not even see what I referred the man for. He focuses on the equally-concerning macules, and making short shrift, dismisses them outright. I wonder if the patient has the nous to realise the barnacle in the room may have miraculously dodged the digital data stream. I move on in a professional frenzy. What can one expect working in a system with a safety net like an abyss? In the NHS we trust.
Mr Heart-Failed Octogenarian
An intelligent man whom I saw in late April this year. A minor chest infection. Treated simply and efficiently with a penicillin. 10 days later he is much better, and unbeknown to me, he is invited to see a modern Florence Nightingale for his spring covid jab. As most his age, he is on about number 10.
He reasonably asks whether it is wise as he is not quite over the chest infection. Florence shoves a thermometer in his ear and pronounces, ‘apyrexial, computer says jab’. This is stupid, since, fevers swing.
That night, his heart packs in. Acute biventricular, congestive heart failure. He is rushed to hospital. He nearly dies. His elderly wife, left alone to manage the fall-out, falls at home and nearly dies in the turmoil of his sudden post-jab turn for the worst.
He only had one serum troponin, which was on the rise. No one in the hospital bothers to do a second. So we will never know if heart failure was induced by a myocardial infarction or myocarditis.
On his ward there is an ostensible influenza outbreak (this is mid-spring). These things didn’t happen like this before the jabs. The reaction is indiscriminately veterinarian. It is to dope everyone on the elderly ward with antivirals. As a consequence (the consultant’s view, not mine), my patient now lapses into renal failure. Still only semi-recovered from the combined traumae of community and hospital healthcare, he is palmed off to the outpatient heart failure nurse. She is similarly algorithmic in her care, ratcheting up the obligatory ACE-inhibitor which does his straining kidneys no favours.
It is a month down the line from me nearly successfully treating this man when I realise after communing lengthily with a computer screen that the rest of the NHS has been misdiagnosing, mistreating and nearly killing him. He looks at me, a shadow, with brain reeling from hypoxia. I am shaking my head in disbelief as I catch up with his exciting month. It is so bad, if it weren’t real, it would be a special kind of hilarious. Black humour hilarious. The kind which makes the ribs and the loins hurt badly. But, it is true. It is also a lot to digest and process in a ten minute appointment.
It is an exhibition par excellence of how to fell a man in several, algorithmic pharmaceutical steps. All without engaging a brain cell. There is no nuance, no rational.
Too many (systemically-blinded) cooks spoil the broth
I turn to him and suggest he must decide if he wants me or the heart failure nurse to manage him. I know I am no longer master of my manor. There are many, new less experienced squires on the plural pastures of mechanised medicine. He looks at me without any deliberation and nominates me. I am almost flattered, but it was, for most of my career, my professional privilege to lead patient care until covid came.
Heart failure nurse nearly has a heart attack. She claims there is conflicting advice. There wasn’t really. She was treating past numbers and applying non-holistic, rigid protocol. I was individually treating the current patient, holistically. I commit no crime. The compliance-algorithm nurse is very angry. She says to the patient she will speak to my junior doctor colleague – the ‘clinical lead’- whom, she was sure, would, quote, ‘fall into line’. As always does she. I have become the problem, since, I think, analyse and question in the best interests of patients. Thus, I am no longer welcome in general practice. It has become an extremist cult of medicalism. No evidence, no experience, only obedience required. A health system for hacks, managers and their superiors, not for doctors, nor even patients.
At this point no one in the NHS is properly engaging the brains which were systematically disengaged by relentless government and media covid propaganda. They follow orders, leaving a buried trail of preventable suffering and death behind them. There is an additional queer NHS phenomenon. In their letters and to patients, my hospital colleagues invariably do not enquire into nor acknowledge the clear temporal relations of the covid jab to the pathology, even if I expressly mention it to them in my referrals. In doing so, they are complicit in forever-rendering the concern impertinent and invisible.
Pemphigus or Pemphigoid: three leaky patients
Mr Bubble Wrap, 80
Early spring 2025, I’m sent to a local care home to see a man with multiple unexplained blisters. Relapsing, remitting and migrating all over his body in a seemingly random sequence. Mmmh, Pemphigus or Pemphigoid? Odd. I begin the usual experiments with various topical and then oral treatments, scratching my head, finally ending in oral steroids as usual last resort. They work temporarily, but as soon as they are removed, out crop the blisters, again. He is put on a metaphorical slow boat to China in search of a dermatologist.
I return 4 weeks later for a seemingly unrelated matter and realise the close, unusual connection between the 10th covid jab instalment and a second patient in the same nursing home.
Mrs Blister Pack, 89
She is the second post 10th jab pemphigoid occurring in the same nursing home, with the jab having been given by the same oblivious nurse, on the same day. This patient had been managed in parallel by a colleague, siloed from my independent observations – both eventually fail to resolve with standard diagnoses and treatments. It leaves the vax as a culprit.
There’s no use climbing the walls about it anymore. Nothing happened at the start. Nothing will happen now. There is every likelihood the observant, on-point doctor announcing a correlation will again be treated like a criminal or a front running candidate for a lunatic asylum.
Yellow card ADRs are, as usual, recorded by me. But, nothing has changed. Nothing will. There was enough concern to pull the jabs before rollout, and more after jabs 1 and 2. We’re on jab 10, and it has long become a lobotomised, continuing assault on the old, uninformed, and vulnerable.
Mrs Bullous Pemphigoid Jr, The Third, 83
A third patient with the leaky dermis. She is an earlier precedent, who comes 6 weeks after, and confirms my hunches on the other two leakers. A dermatologist-diagnosed case of bullous pemphigoid, after the first two jabs. She has been on on a constant trickle of oral steroids since 2022.
The greater tragedy is that she is continuing to have each and every jab offered up to her. I mention very innocently the pattern of dermal leakiness I have noticed. The attendant daughter, not that shocked, takes the hint and seems, with her body language, to indicate things might be different next time. I ask her to give my regards to her mother’s dermatologist.
Leaked truths
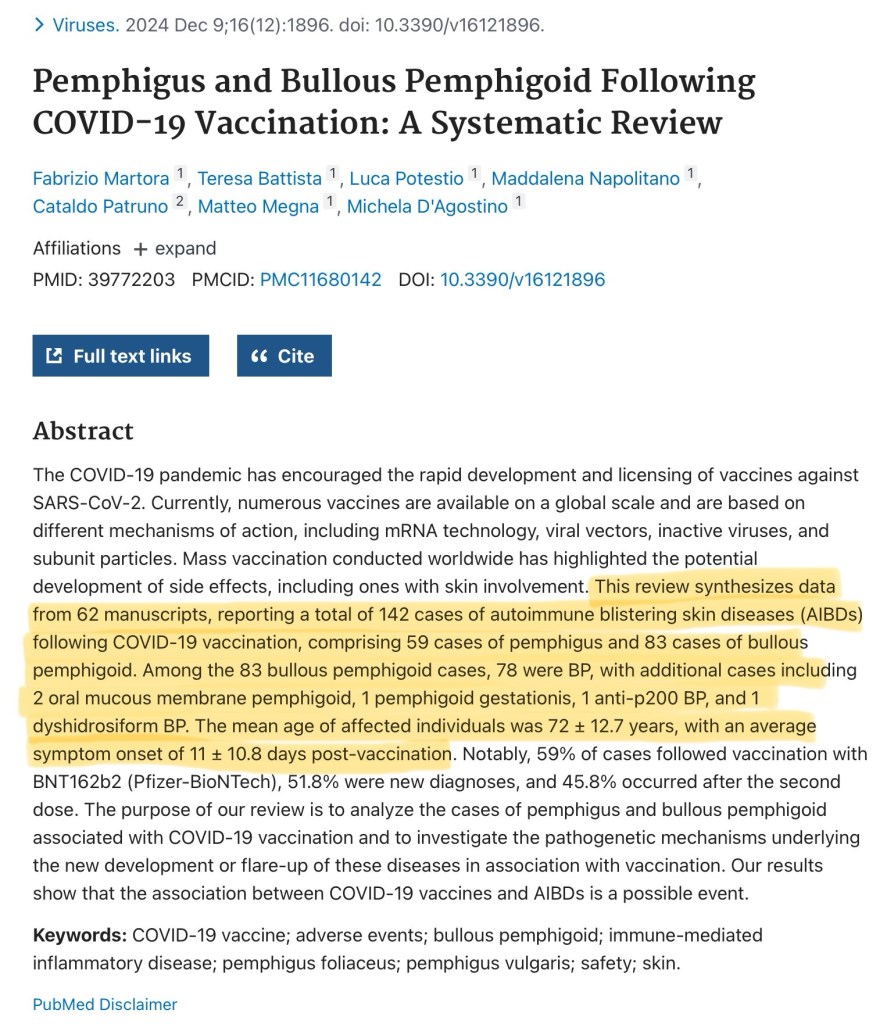
Finally, as it used to be pre-2020 and before the scandalous propaganda of the MHRA. Professional Life mirrors clinical research. At last, there are cracks appearing in the dam of lies erected against research leaking truths, published in an academic paper:
“Pemphigus and Bullous Pemphigoid Following COVID-19 Vaccination: A Systematic Review: This review synthesises data from 62 manuscripts, reporting a total of 142 cases of autoimmune blistering skin diseases (AIBDs) following COVID-19 vaccination, comprising 59 cases of pemphigus and 83 cases of bullous pemphigoid. Among the 83 bullous pemphigoid cases, 78 were BP, with additional cases including 2 oral mucous membrane pemphigoid, 1 pemphigoid gestationis, 1 anti-p200 BP, and 1 dyshidrosiform BP. The mean age of affected”
The Creaky Carer, 60
This 60 year old care home worker, had 2 jabs under State duress of destitution, and now embodies late-onset inflammatory arthritis and a lifetime anchored to expensive blockbuster biologic injections. She dares to say, ‘may I ask if it could be the covid jabs?’ because most likely, she has heard I am even open to very reasonable questions. I affirm her question. By running through the research and my own clinical experience, I absolve myself of professional quackery.
There are many of these demographic autoimmune disease anomalies since covid injections. Untimely, unusual, unnecessary. But not now unexpected. Sadly, the rheumatologists in hospitals act like it is normal. Never once taking a recent jab history, never once questioning the new abnormal. They must be seeing more concentrated series of abnormalities than me. I am subversive, the patient is questioning. I suggest when she sees the expert to ask the obvious, unmentionable question on all sufferers’ lips: could it be the jab?
Young Farmer Angina, 43
A non-smoker, a wife and two young children. In the end I have to admit however unlikely it used to be, this formerly very active, physically fit man may have severe angina. Rapid Access Chest Pain Clinic, here we come. He regrets having the first three jabs and he loathes the government for, after destroying the medical profession through covid, destroying farmers through taxation. In any case, he is no longer fit enough to run his own farm. The State are belt and bracing his destruction.
This 2025 pre-print on, ‘The intracellular aggregation of encoded spike monomers and their subunits as a cause of cardiac side effects’ states:
‘The arrangement of these complexes always adhered to a consistent pattern in each cell type. Particularly in AC16 cardiomyocytes, the various spike protein derivatives impaired not only cell proliferation, but also induced a pro-inflammatory response and oxidative stress.’
Ms Croaky, 75
An acute dysphonia and pyrexia two days post-jab – is it a coincidental laryngitis, or is it something else? Could it be post-covid jab ?(herpetic) recurrent laryngeal nerve palsy? These days it is all on the cards.
Mr Another Seventy-something
Another seventy something. Five days post-jab in the left deltoid, he develops symptoms of an ipsilateral arm, brachial plexitis. Oh well, we’ll just have to see what happens… what else is there to do?
In-the-know Farmer’s Wife, 77
Farmer’s wife is asking after her delayed replacement hip operation. A hip well-worn proving a life well-lived. Hip aside, and as if to mitigate her one weakness, and without being led, she spontaneously says she has been as ‘Fit as a fiddle in the last 5 years, and I’ve not had one of those jabs … I know what’s in them’. Actually, I’m sure that she does not, but I know what she means. She appears as a rare apparition sent by the universe to fortify me in a lonely plight.
Mrs Unseasonal Pneumonia, 76
It is late spring, 2025. She nonchalantly has 10th jab. I comment equally nonchalantly at the un-seasonality of Mrs Unseasonal’s pneumonia. Breaking into what is altogether an uncharacteristic u-turn, she cocks her head professorially, ‘I have noticed that in other people. I ONLY got chest infections at winter before.’ However, she carried on jabbing, being the trooper she is.
‘I guess you have to balance the risks,’ I say charitably; and in concession, ‘they do peddle it by saying you could be worse without it.’ Before biting, ‘But, some of us have not had one and not been ill in 5 years.’ Says I, who has been on the faux frontline of nothing in particular, facing these coughing, spluttering, covid PCR positive masses.
Mr Chesty Nonagenarian
On the same day, a 93 year old man, with a similar ruttle, since a week or so after a COVID booster in the residential home. Chesty, and breathless. I sardonically point out and underline the close correlation to the attending care staff, who already know this correlates. The covid jab seems at once a slow-kill, fast kill method, all locked in by fear of a worse death, or of reprisals.
Mr Chesty is too demented to take the hint, so he will progress to the 11th booster level and by then we will again be at the gates of winter, and he will have to contend with the combination of the triple-whammy: jabs of flu, covid and the winter. This may well be the mortal blow. The irony that he may have jab-induced dementia is not lost. The research data on spike protein-induced neurological damage continues to accrue, as in this paper, but, true to the wilful blindness we have become accustomed to in tyranny, not once do the researchers dare mention damage-potential via injected spike protein gene templates.
potential genotoxic, and therefore neoplastic risks of bio-engineered viral spike protein. These academic rascals cannot allow themselves to inevitably extend their conclusion towards the bio-engineered spike protein gene vaccines.
Mrs Ever-Thinning, 75
Mid-June 2025, retired, widowed, fading away for about 18 months to 2 years, weight dropping, total serum protein falling. Body scan shows no cancer. Bloods, essentially otherwise unremarkable. After the tenth covid booster, she collapses, and receives seven stitches to the forehead. The shocking blood pressure of 80/40 is deemed ‘her baseline’ by A&E. Contradicting the emergency doctor’s narrative of convenience is the action of 250ml of intravenous fluid bolus to resuscitate her before a CT scan.
She is sent home with a low serum potassium of 3.2 and hypotensive. Barely able to lie back in her bed. A concerned district nurse calls me in, her standing systolic blood pressure is 67. I ask if she felt unwell after the covid booster? No, she replies. Yet, 48 hours later she did collapse.
The CT scan demonstrates some ground glass opacities in the chest, with a plan to repeat the scan in three months. That is all. After this gross incompetence, is it worth or is it safe sending her back? Lord knows. I try again to point out the obvious in a hurriedly scribbled letter to my colleagues and hope for the best as I call another ambulance.
She is skeletal, slowly, indefinably and non-specifically wasting away. No one can work out why there is a non-specific slow change in one lung base, she is too weak for a bronchoscopy. Yet, she dutifully has every covid booster. One wonders what could have been had she not. We will never know. We are where we are. She feels they are safe, effective and necessary – but for whom?
I want to tell her to stop, but I know she is so locked in and so obedient to the State, in the way only a lifer in the teaching profession might be. She would consider the very suggestion a call to death, not life. At best, it would confuse, anger and distress her. So, the death spiral continues spiralling.
Mrs Relatively Frank-Clot, 83
She had a pulmonary embolism after the her fifth and final jab. She is on permanent anti-coagulation. She stopped having jabs. In a remarkable and rare moment of clarity, she reports she was told by her hospital doctor, ‘They could not rule out a link.’ This is more honesty from a doctor than most have received.
‘The consistent subclinical changes in inflammatory and coagulation markers suggest that these pathways may be involved in the pathogenesis of severe ARFIs [sic] (adverse events following immunization) reported with mRNA vaccines.’
Mr Another-Weird Post-Jab Rash, 81
He is sent an SMS call to covid arms. He dutifully answers it. Two weeks post-10th covid booster, he develops an atypical evolving, migratory generalised inflamed, itchy red discoid rash to his upper back, the left upper arm and right lateral calf; there is a danger at the leg and upper arm of the skin eroding and becoming infected. I turn up the steroids, and note the developing patient series of post covid jab dermatological pathology.
Ms Secondarily Infertile, 29
Two times Pfizer in mid-2021. Never returned for the third because her periods stopped somewhere between the 1st and 2nd jabs, and for over a year. Eventually they returned, then she miscarried. She is desperate for a child. Her leaders are desperate for her to not. Her pregnancy is officially unsustainable. The young couple have, since, been unable to conceive for two years. Time has made her candid. Today, she says she believes it was the jabs. Professional experience tells me this is reasonable. What else is more likely?
‘Successful conception rates were substantially lower for women vaccinated against COVID-19 before successful conception than for those who were not vaccinated.’
Little Miss Arthritic, 18
Three years of paediatric joint issues. On examination, an acute-on-chronic polyarthritis with raised of CRP 57 and a rheumatoid factor of 39. She cannot recall if she had any vaccines around the time of onset. Yet, she did, in October 2021. When reminded, she cannot recall any issues with it. Yet, for some reason, even unbeknown to her, she did not complete the course of two. She does not seem to care. She, instead and without basis nor correlation in time, wonders if a hormonal implant 8 weeks ago has anything to do with the 3 year illness.
Celtic Mother Earth Figure, 54
She is feeling fatigued these days. She arrives, with big hopes. She wants to be tested for every vitamin and mineral known to man. She’s there to fine tune her health to perfection. I drop it gently that there’s no way the NHS will provide all that, but I’ll do what I can. Such was her interest in perfect health, that, as she stands to leave I ask, in fascination, ‘did you have any of the covid vaccines?’
She stops, her face drops, her shoulders round and she hunches her back and almost dissembles, ‘Unfortunately I had three. I wish I’d never had any… but I didn’t know then… and I’d had a bad flu… and I have a (minor) chest condition.’ It seems she had rehearsed her excuses very well, but, there was the concealed, deep regret many now have. I commiserate her, ‘Some people are still having them, on number 10 or 11.’ We bid farewell. I have a queasy suspicion she led her little girl down the same path.
Five and a half years later, in spite of desperate continuing and current attempts to resuscitate COVID-19 pandemics, there was and is no justification for giving unnecessary, unsafe and ineffective jabs.
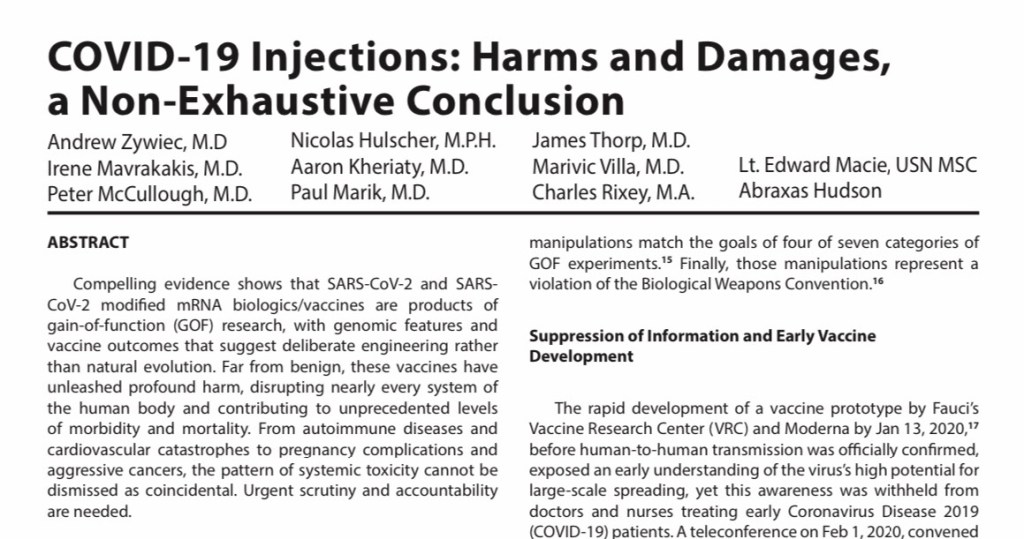
“IRREFUTABLE Grounds for Immediate Market Withdrawal of COVID-19 mRNA Injections,”
“Together, the international evidence has converged: mRNA injections are unsafe, ineffective, contaminated, and in violation of international law,”
McCullough et al continue to add to the ever-increasing pile of indictment ignored by institutional blindness and wilful obfuscation.
The crime of covid jabbing continues to be perpetrated by casual, normalised NHS hands which themselves would now, never wish to receive in kind. The continuing crime scene is now geriatric, mainly confined to care homes, the demented, and institutionally-ignorant. Also, those extremely scared of death and dying but nonetheless not of iatrogenic illness and death. Then, in contrast, there are the journeymen patients who take the multiple jabs like a well-worn punchbag, they neither seem to flourish nor perish. It is also true to say, that I have countless more patients who by being unwell call into question the jabs. My current enumeration of cases is not by any means exhaustive.
Newsflash
In the last week of August, a message flashes up on the screen. A colleague leading the charge in the old people’s homes:
[BANZAI!] Warning, 9 residents just tested positive for COVID.
I couldn’t care less. What does that mean? Does it mean they are unwell? Does it mean testing is meaningless? Does it mean the ongoing jab campaign is not only dangerous but futile?
I shrug and carry on. It is a continuing human folly I want no part of. To me the implied disaster is unlikely, in a hot summer, and there has been a trend this season for patients and carers to start testing again. There is no real disaster on the ground apart from the population being more unwell than before the jabs, with strange disease outbreaks following each round of jabs. The less jabs, the less disease. I do wish they would stop it.
So, what actually is ‘covid’? It is an excuse of quickly transforming the relationship of the State to the individual into a tyranny in order to implement whatever change the controllers of the States wish.
Will we ever emerge from World War III?
Epilogue – A Brief Encounter
Dr Confessional Purgatory, FRCGP, late 50s
GP appraisal, late 2025. A process ushered in by a serial killer colleague. Intended to prevent sociopathic killers entering the profession. It doesn’t. It helps hide them. For, the exercise is one of decerebrated regulatory compliance. One witnessed the dark place this precise, obedient attitude dragged the profession during covid.
My appraiser, a very senior colleague, perhaps in her late 50s, provides a sad end to the proceedings. The process has been abstracted into an on-line platform because of covid, and remained there. Over three years, I have been incrementally stretching her tolerance with allusions to covidology. Each year she has smiled benignly, and once even dared ask my covid vaccination status. My reply was a polite, Foxtrot Oscar.
This year, she emails last-minute: Not enough evidence of CPD (continuing professional development) to pass go. I have plenty of evidence, but it is all taboo. I determine to let rip. I apprised her of recent research discussing dermatological and cognitive disease potentially caused by ‘covid gene immunotherapy injections’. In my portfolio, I dispense with the use of the vernacular ‘jab’, but cannot bring myself even in this confessional torture chamber call them ‘vaccines’.
Last year, I had gently alluded to cardiac, thromboembolic and cancer concerns. Today, I am prepared to be severely challenged over stretching her dogma to the limits. I am taken aback by the response:
She says, You know, you go into things in such depth. I have a learned a lot from you in the last three years. I will miss our meetings… I’ve had heart problems in the last two years and now I have a pacemaker and it’s not really relieving my symptoms of fatigue properly. My blood pressure drops and I feel terrible but they tell me everything is fine. And my partner, well he’s young and he’s developed cancer in the last two years, and it’s only since he’s had these jabs…had chemotherapy… and he’s so frightened, he keeps having the covid boosters. He’s on number 10. And… you know, funny you should mention it… his memory… his memory isn’t as good as it used to be… me and my son, he’s also a GP, we’re wondering whether it’s a good or bad thing.
She mentions that there was a young doctor at the practice where she is a partner who refused to have any of the covid vaccinations, as if it was somehow abnormal. It was, clearly, not absurd. I reply, ‘that seems to be a sensible response given it used to take 10 or 15 years to develop a vaccine, and that, allegedly, this one took six to eight months.’ I mention that one of my relatives is a pharmaceutical chemist and works in the regulatory aspects of gene therapy, to back the statement up.
It’s our last of three years of appraisals, and my appraiser bids a slightly emotional farewell. She looks more tired than at the start, having forcibly been slid into semi-retirement by ill health. Slim, but sarcopenic; receded, impossibly-dyed hair line and a droplet-belly belying a weak core. It is a tragic picture. Frankly, she looks knackered.
She says, ‘Well, I’ve learned a lot from you. It’s been an education.’
Has it?
You’re an unusual person? You are… ummmh… errr… eccentric.’
‘Let me help you. What you’re trying to say is I am abnormal.’
‘Yes, actually. Perhaps you’ve got something like ADHD or Asperger’s… you go into so much… detail.’
Her statements speaks volumes about the profession, where it is, and why it cannot change direction. It is medicalising, and therefore making abnormal the quality of basic competence. It is defeated, unwell and confused.
She continues to ramble, ‘My partner, we’re not sure what he should do about upcoming (11th) covid vaccine… but I think I’ll have the flu jab and I think he will, too.’ They remain trapped between a rock and a hard belief. Could she not see the pattern for herself in her privileged daily position in front of her damaged patients? My patients could.
I almost cannot contain my astonishment, ‘Well whatever you do, don’t have both together on the same day,’ and I, jaw now suitably loosened by her candidness, reiterate the horror of what happened in my practice, Christmas 2022.
She looks helpless, confused and trapped. I try help her out, ‘Well, I’m not really sure what’s going on but it’s a really difficult position when the State says one thing and your patient and you know a different thing… I guess we’re all prisoners of our own Truths.’
‘Yes, yes,’ she nods fervently. She again mentions that she has learned so much from me in the last three years. This continues to shock me, as we both accept that a misfit like me would never be allowed to be a leader in our profession of medicine. She has been extraordinarily helpful and kind over three years as my appraiser, sensing that I was different, from the off.
Finally, Like a scene from a Brief Encounter. There is a rapid gushing of yet, unrequited words. A quick transfer of ‘turbo cancer, SV40, DNA contamination, Angus Dalgleish’, and a final turn of heads in the night, amidst the steam and whistle, to frantically wave and shout, ‘Use Yandex, or you’ll get Google-Nowhere!’ It is The End of The Affair.
This is the frank, urgent interchange between medical colleagues that should have occurred everywhere, five years ago. Yet the profession is still siloed in the comfortably dumb bunkers of medical normalcy. For me, these medics may have been so deeply entrenched in a superficial denial of in-the-face facts, they put short-term individual survival in front of long-term collective benefit.
For five years, a minority of doctors and patients have privately been meeting to whisper, some individually publicly screaming in pain and being correspondingly severely punished. Sometimes they have written and published, secretly, for the best interests of everyone. They have been roundly berated for consistently being proven, in real terms, correct. Our brethren have remained in the trenches, as major opposition. Finally, they begin to openly ponder surrender, of coming up for air, of raising white flag and daring to admit self-harm, of aiding and abetting the harm of others.
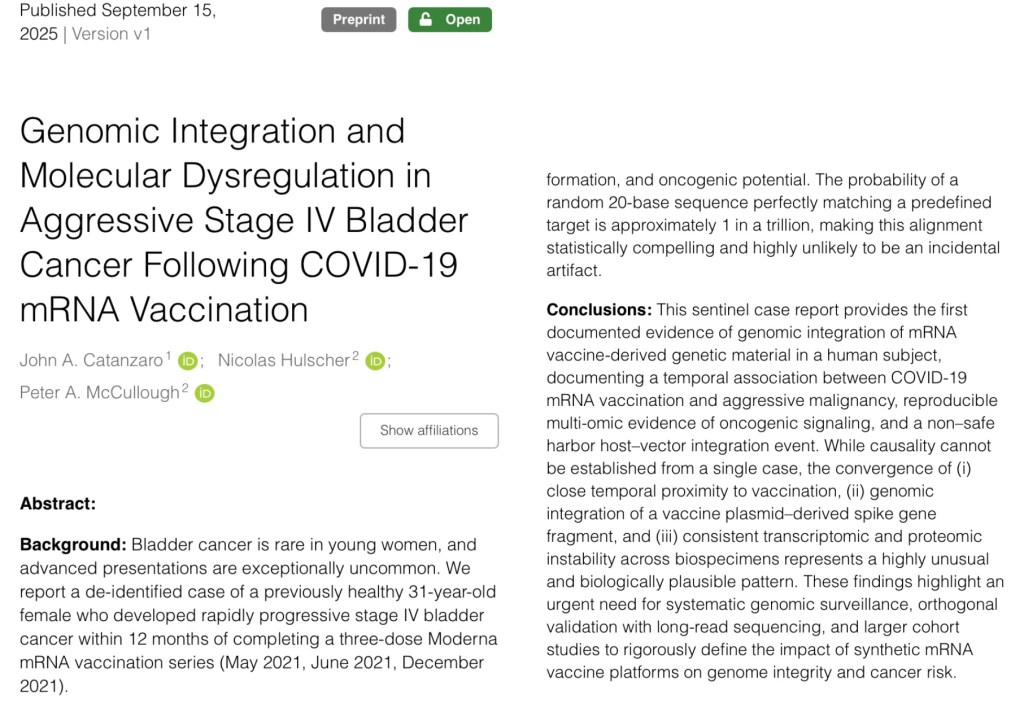
15.9.25McCullough et al: “This sentinel case report [healthy 31 year female] provides the first documented evidence of genomic integration of mRNA vaccine-derived genetic material in a human subject, documenting a temporal association between COVID-19 mRNA vaccination and aggressive malignancy, reproducible multi-omic evidence of oncogenic signaling, and a non–safe harbor host–vector integration event.” Source & Preprint
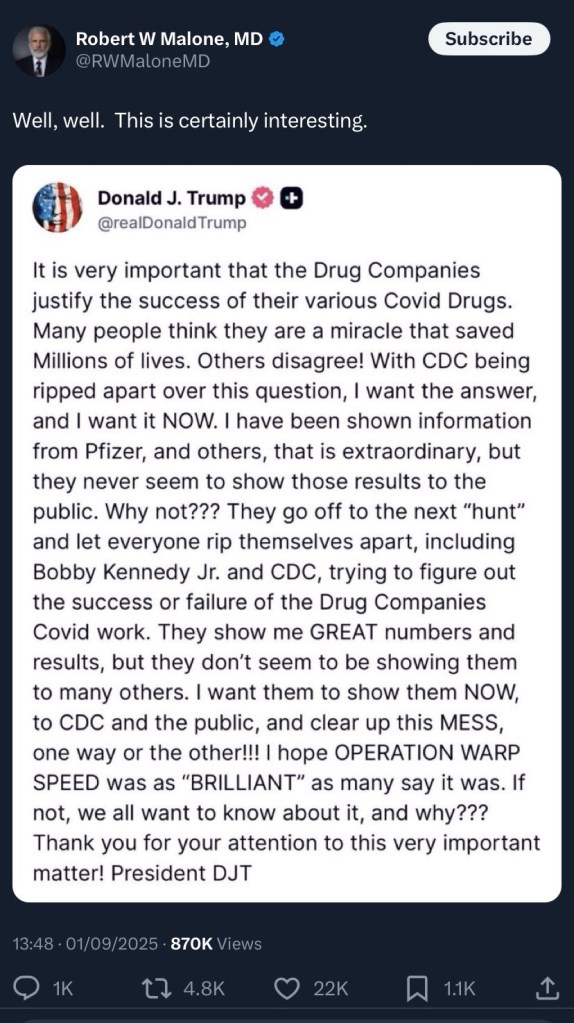
1.9.25Bread and circuses:Doublespeak from Warp-speed POTUS Mr. DJ Maverick Flip-Flop Puppet. Do not hold your breath. We are due a SPARS pandemic. Source: X
”One of Britain’s most eminent oncologists, Prof Angus Dalgleish, said for me to share with you today that he thinks it’s highly likely that the Covid vaccines have been a factor, a significant factor, in the cancer of members of the Royal family.”
3.9.2025 Surgeon General Dr. Joseph Ladapo Announced That Florida is Ending Mandates for ALL Vaccines, “Every last one is wrong … Who am I, or anyone else, to tell you what you should put in your body? Who am I to tell you what your child should put in their body?” Indeed.
8.9.25The United Confusional States of America:Trump’s recent thimerosal remarks will be used to promote the alternative, poisonous modified mRNA injections, and may not at all achieve redress for the dead and damaged.
Please let me know in the comments about your own, related experiences. Please share this with your doctor, and let me know the response.
19th September 2025
All links are archived and if broken may, in the majority, be found by searching the link onarchive.isor, in the small minority, onweb.archive.org.
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, asprescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
Thank you TCP for recording and continuing to talk and write about this on-going devastation with the covid jabs. I know it must be very hard on your spirit and well-being to be managing this on a daily basis. Each of these patients is fortunate to have your integrity and knowledge to support where you can. I think we are all continuing to see and hear about medical challenges and deaths very likely from the jabs even with people who have stopped getting them. You have enlightened me. I had no idea that so many vulnerable seniors are on their 10th or 11th shot. So much harm, physical, phycological and financial trauma resulting to people and families of all ages. Take Care


Sic transit gloria mundi… Take care, sad to say, but on the button.
LikeLiked by 1 person
Thank you TCP for recording and continuing to talk and write about this on-going devastation with the covid jabs. I know it must be very hard on your spirit and well-being to be managing this on a daily basis. Each of these patients is fortunate to have your integrity and knowledge to support where you can. I think we are all continuing to see and hear about medical challenges and deaths very likely from the jabs even with people who have stopped getting them. You have enlightened me. I had no idea that so many vulnerable seniors are on their 10th or 11th shot. So much harm, physical, phycological and financial trauma resulting to people and families of all ages. Take Care
LikeLiked by 1 person