Some decades ago, there was a weekly column in The Spectator. When the inebriated columnist, gripped in his local Victorian London pub by a hepatic illness of his own making was unable to write, in lieu of the absent column appeared his doctor’s sick-note: JEFFREY BERNARD IS UNWELL.
SO IS TCP. Most especially after reading the excellent, on-point but extremely depressing histopathological autopsy cases in, VACCINATED – DEAD.
Unlike Mr Bernard, the self-cure for TCP is an expurgating dose of book review, and not like Jeffrey, tumbling back into Soho after a few.
This slim, but densely factual and telling atlas of cases is the most damning indictment of covid jabs’ killing powers. It is written in translation from the original German by colleagues of the Late Professor Arne Burkhardt. He was a pathologist who came out of retirement to discern the pathological truth of the numerous deaths happening in shocking synchronicity and too close in time and space to the purported lifesaving covid jabs.
The continuing, systematised whitewashing, suppression and concealing of the immediately-apparent, gruesome truth of the fast-tracked jabs remains more shocking.
The book is the very information I and like-minded physicians needed in 2021 to confirm and encourage further disclosure of what we already thought we knew, until the government made with multiple sophisticated menaces and misinformations the opposite to be believed.
Instead, the devils of the mafia-enabling MHRA, Ofcom, GMC and the propaganda machine formerly known as journalism conspired with our public health officials against public health. The world has forgotten the woman who steered the General Medical Council during covid on a suicide course to destroy medicine was former paediatrician and GMC Chair, the Late Dame Clare Marx.
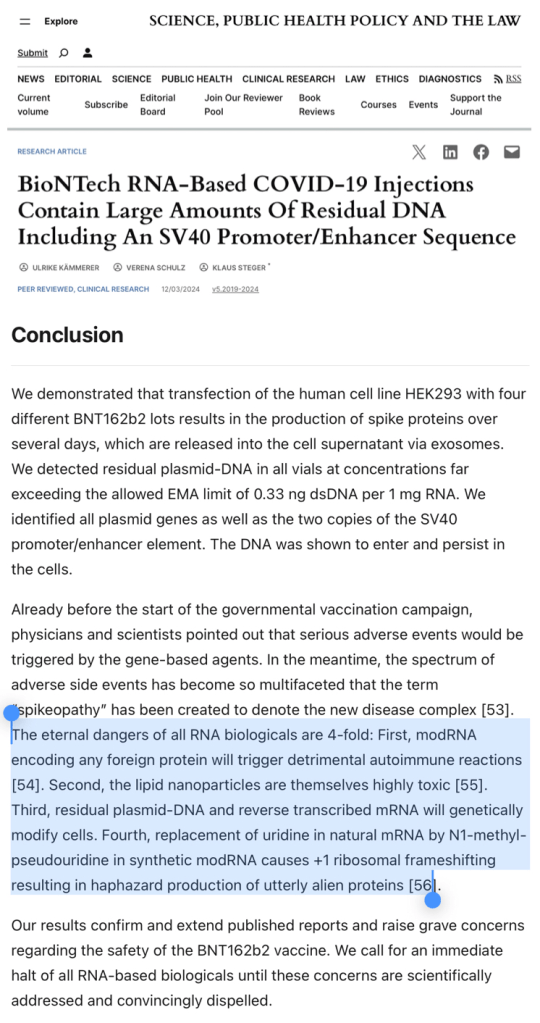
She stepped down in July 2021 following a diagnosis of pancreatic cancer, finally dying in late November 2022. She would have been at least double-jabbed, by then. It would verily be supreme tragic irony if she in fact succumbed to SV40 and DNA contaminated COVID-19 ‘vaccines’ via any of the 13 carcinogenic mechanisms proposed by Professor Angus Dalgleish. Yet, her successor and her organisation continue, as headless chickens unable or unwilling to gain proper perspective of the crime they, at once, are part of and which they part oversee.
Oncologist Professor Angus Dalgleish has exposed 13 mechanisms by which mRNA vaccines may induce or promote cancer, any one of which should have triggered an immediate ban.
Many Germanic Heroes
Professor Lang and Ute Kruger should be guests on every source and form of mainstream and social media decrying the crime. The reality is closer to the new normal: no one knows, no one cares, and the covid measures mass democide is overshadowed by the same actors creating multiple theatre wars and an ethnic-cleansing by genocide for their continuing pecuniary gain.
The book is sombre and sobering reading. In particular for one who has witnessed the sordid unfolding of this massive medical lie within thousands of patient consultations over five years.
It is a definitive handbook for the histopathological causes of the in vivo, realtime pathology one witnessed in ones’ poor, preternaturally terrified, but hopeful patients. Those who queued for miles around the corner for their lives to be saved by the medical and nursing professions. How many queued for their premature and predictable deaths?
This scientific analysis makes one think even more died than the extraordinary mass killing one had already apprehended and foresaw.
To see the case reports of these poor, dead and often young humans alongside the photographs of their histological tissue samples contextualised by the clear relationship in time, space and pathological mechanism to covid jabs makes for a profoundly distressing read.
The basic method, as with the most graceful medical and scientific proofs is, on the face, simple. Immunochemical staining of the damaged tissues with spike protein but not nucleocapsid protein is reasonably presumed to be damage by injected, pharmaceutical modified mRNA, and not by the elusive SARS-COV-2 purported to be the product of US funded gain-of-function bioweapon research.
The consistent presence of the unusual so-called ‘white clots’ reported by embalmers everywhere, resonates with the coagulated masses of blood-pauce fibrin found by this team. Amyloid-like deposits – about which I have written of as a possible cause of an emerging neuropsychiatric pandemic – and unexpected, dark inorganic, carbonaceous crystalline matter deeply sequestered in multiple human organs of the same cadavers abound as indelible evidences of a very peculiar, multiple homicide international crime scene.
The dark organic matter is notable, for the good pathologists leaving it there. However, anyone in the know realises the inference: injectable graphene derivatives and nanotechnology. Once one has evaded or waded through the swamp of misinformation laid by Google, one easily sees graphene oxide is an object of pharmaceutical interest for its cytotoxic and inflammatory effects.
Indeed, if it is pro-inflammatory (it is), it is an experimental candidate for a vaccine adjuvant. See this 2016 lecture on Cellular Responses to Graphene Oxide Sheets by Dr Sandra Vranic at CLINAM (European Foundation for Clinical Nanomedicine), Basel.
The bluetooth coupling, magnetic deltoids do not seem so conspiratorial, now. Particularly, in light of the numerous patents and university departments outlining such things. We now know for sure that graphene oxide has been discussed as a vaccine excipient precisely for its pro-inflammatory nature.
One recalls the German scientist Dr Andreas Noack (who claimed his PhD included the conversion of graphene oxide into graphene hydroxide). This man was an expert in graphene and its derivatives, and his righteous indignation at the covid jab crime led to a live-streamed raid by armed German police upon his home. Sometime later he suffered an untimely death in the arms of his pregnant wife. It was convenient for only those wishing to suppress the man’s expert truths.
Germans not only figure prominently in the State implementation of covid-related mass denials of liberties and bodily autonomy, but also in their fine antagonists. Think of Drs Wolfgang Wodarg, Sucharit Bhakdi, Heiko Schöning, Reiner Fuellmich, and MichaelPalmer. Nearby, across the Alps was Swiss cardiologist, Dr Thomas Binder, preposterously detained under the mental heath act for pointing out the obvious concerns of the covid narrative. All at some point were ostracised, arrested, charged and/or jailed, and one even labelled the most specious of curses, anti-semite.
Dr Thomas Jendges, a leading German doctor became a casualty of the covid era after he fell from his hospital rooftop in an alleged suicide. Despite Reuters best attempts to debunk this by loosely associating one wild report with other more based reports, Lord Mayor Sven Schulze said on the morning of 2.11.2021:
“It was with great dismay that I had just learned of the tragic death of Dr. Thomas Jendges, the managing director of our hospital. Just last night we exchanged ideas for a long time about the difficult corona situation.”
He just happened to leap off the hospital rooftop a few hours later. Doctors do this all the time. Move on. Nothing to see here? Dr Rose furnished us with more, as did Stess News, and Las Republicas.
In recent German elections, 16 candidates, including 7 AfD members died just before polling. Dr Fuellmich was politically active in Germany with die Basis. He was a powerful and eloquent counter voice until he was detained in Mexico and extradited to Germany. The detention increasingly looks not only like injustice but a deliberate State attempt to silence him by politically imprisonment. It has worked. He has a successful record of bring fascist corporations to heel and legal account. No doubt he would have done the same to Pfizer and Co. All chance?
Further clinical coincidences come thick and fast reading Vaccinated – Dead.
Vaccinated – Dead documents a pandemic of clinicians overlooking the obvious temporal correlation of covid jabbing with acute and chronic morbidity and mortality. Then, a laundering of that with nonchalant primary autopsy diagnoses in silenced, jabbed corpses, each inexplicably riddled with unusual, co-existing, multiple pathologies.
Suspicious, bereaved families sought secondary histopathological examinations. These uncovered physical evidence of multiple, strange, and sometimes novel findings entwined in a murderous noose of amyloid-like, fibrin, and black, crystalloid, carbonaceous deposits. Threads sodden with liberal doses of multi-system lymphocytic infiltrates, all immunohistochemically linked to covid jabs.
How my own extraordinary clinical observations as a lowly, lonely clinician somewhere off the continent can so closely mirror my German laboratory colleagues’ is (to paraphrase Fleming) not mere happenstance, and not even coincidence, it implies enemy action.
Casebook Examples
Cardiovascular pathology
Take, for instance, my young female patient with a very rare case of post-covid injection aortitis in 2022.
There are several aortitis cases and many cases of cardiovascular system inflammation and thromboembolic disease in this book. They ably provide convincing pathological bases of modified mRNA injectables driving disease and death.
Take, for example:
Case 10, page 79, dead 61y male: aortitis, aortic dissection with wall rupture, pericardial tamponade, massive vasculitis prostatitis. I recall vividly my friend’s relative, a mid 40s male inexplicable developing acute urinary retention a week or so after his first covid jab in early 2021;
Case 66, page 35, died suddenly on a park bench after surfing, 48y male: aortitis, pericarditis, thickened pericardium with amyloid-like characteristics, myocarditis with loose interstitial scarring & amyloid-like characteristics;
Case 17, page 24 & 25, dead 83y female: multiple myocardial black, crystalline deposits of uncertain origin, some needle-like, often with corkscrew-like ends;
Three siblings near-simultaneously falling ill, two victim to serious cardiovascular events in December 2022.
Dermatological pathology (with Clots, Vasculitis and Hypertension)
Case 39B, page 22, 127 & 128, 43y female: blood sample containing homogeneous, non-layered fibrin thrombus… vascular changes are well compatible with the clinical finding of increased peripheral resistance in the capillary bed [ie a risk factor for hypertension]… amyloid deposits in the vessel walls… perivascular lymphocytic vasculitis… significant proliferation of dendritic cells in the epidermis;
Case 113B, page 29 &129, 38y male: cough, pleuritic chest pain, headache, brain fog; significant rarefaction of basement membrane elastic fibres… disruption and fragmentation of elastic fibres within the deeper dermis;
I refer you to:
The general rising pathology and inexplicable severe hypertension cases I reported in 2022.
Case 42, page 94, dead 84y female: admitted for shingles following her 1st jab, only to be opportunistically diagnosed with asymptomatic covid in the hospital; she was most likely given a ‘curative’ second jab by the hospital, only to die 17-33 days after discharge;
Case 42 typifies the murderous pandemic of State-sponsored wrong-thinking and wrongdoing which is increasingly occurring all over the Western world. See my 88y patient with recurrent post-jab shingles in November 2021.
Neurological pathology
Case 60, page 53, dead 72y female: brain haemorrhages, inflammatory changes, infarction with partially dilated blood filled vessels with surrounding lymphocytic infiltrate, patchy fresh haemorrhages. Amyloid-like hyaline material in the brain blood vessel walls;
Case 120B, page 129, 63y female, presented with hemiparesis, ataxia, character change: encephalitis, brain vasculitis, amyloid-like brain deposits, lymphocytic & phagocytic infiltrates;
I have written in detail regarding my clinical experience and emerging suggesting covid jabs are associated with increasing prevalence and prematurity of chronic neurological illness and cognitive impairment in March 2025.
Gonadal pathology (with Myocarditis and Clots)
Case 18, page 66, dead 29y male: disorder of spermatogenesis,
Case 56, page 65, dead 85y male: lymphocytic testicular inflammation;
Case 157A, page 132, 15/40 abortion material (after intra-uterine death): both father and mother triple vaccinated; Gravida 5, Para 1 mother gave birth in 2018, but subsequent 4 unsuccessful pregnancies inter- and post-covid jabs. Spike protein positive, nucleocapsid negative endometrium;
Case 159, page 31, dead 16y female: myocarditis, subclavian and brachial vein thrombosis, spike protein detected in ovaries;
Here, we have explanations for menstrual disturbances, and miscarriages I noted were occurring uncommonly frequently, and a validation of the officially ignored, logical infertility concerns raised by Drs Wodarg and Yeadon on page 5 of their December 2020 petition, about which I commented, here, also in 2020.
See:
My 36y female patient of November 2021 with post-jab dysfunctional uterine bleeding;
and, my 40y female patient of November 2021 with post-jab secondary amenorrhoea since the second jab.
In fact, I wrote to various government officials in July 2021 warning them that many of the above realised ADRs and disease were occurring, and were highly likely to occur, according to the evidence of that time. In May 2023 I added further concerns regarding post-covid jab related emergent disease patterns.
As with other studies and other clinicians’ reported experiences, my clinical experience corroborates well with the findings of Prof Burkhardt’s team. Experiential evidence of this clinical sort is compelling but continually attacked and ignored. The many post-covid jab deaths were hidden and not flagged by the medical and coronial systems. These deaths were mass-misattributed and fast-tracked to cemeteries by purposely degraded medical and death-certification systems.
Journal of Medical Virology Research paper. Long-covid = Long-vaccinated. Hulsher explains. Anomalous Amyloid Microclots Found in 100% of the COVID-19 Vaccinated. He proposes nattokinase may be therapeutic.
Transthyretin Amyloidosis
Tafamidis, is being pushed under the brand name Vyndaqel by Pfizer for the treatment of transthyretin amyloidosis with cardiomyopathy. This month, I happened to attend a lecture with a Pfizer drug representative advertisement force-fed into the middle if it. The FDA is said to have approved this use in May 2019. This type of amyloid is implicated in multi-system disease and is now being implicated in covid jab pathology. Is this another supreme irony, where Pharma take with both hands, Pfizer jab cardiomyopathy, etc, followed by Pfizer Vyndaqel?
Medical Risk
Prince Monolulu & The Diamond Princess
Vaccinated – Dead is sobering for other reasons. Reading it, one contemplates upon those of my colleagues who were well-meaning but ignorant and propagandised, and their hapless patients.
One thinks of the normalised, inherent danger of old normal medicine. How simple routine procedures can unexpectedly and suddenly bite back, taking the life of a fellow, dear human patient rapidly away to somewhere on an autopsy gurney. The cost of failure is truly dear.
It is painful, because it, once, happened to TCP. No matter what one’s noble intent, no matter the desire to do one’s best for one’s patient, sometimes even in the safest of health systems, it does go catastrophically wrong. One is caught in the eye of a storm in deathly embrace with a patient. One mourns the death more deeply than one’s own blood. It is usually less common than what occurred with global, centrally-cascaded covid measures.
Life is an inherently risky business. Even offering a friend a sweet can be fatal, as Jeffrey Bernard discovered when he offered his unwell, good friend, Prince Monolulu a strawberry cream chocolate. Whilst, sat beside the hospital cot, he wished him better health. This fraternal action turned the cot immediately into his now choking friend’s deathbed. Presumably, there was no intent to kill in this ritual act of brotherly nourishment, proffered from a deadly box of ironic Black Magic chocolates.
Dealing in the voodoo of medical cures often carries the heaviest risk of death, as this doctor learned at a heavy, lifelong cost. We are forever on the cusp of ending a life on the end of a needle or the nib of a penned prescription for oral penicillin. Even the most successful scalpel can end down the road in sepsis and premature, unexpected death.
How many has one killed but not even realised?
However, covid has ushered in a new era of carelessness so reckless it is tantamount to intent, negligence so bad it is manslaughter. The act of the State-suppressing knowledge that covid jabs were so seriously harmful is so bad that government officials’ actions and inactions are complicities in mass medical murder.
Most disturbingly of all, in spite of all the facts, this poisonous mixture continues to be purveyed to selected vulnerable individuals. It is as if those who commit the crime hide it by attempting a slow, imperceptible retreat, killing as they slither away.
It is said each doctor has a cemetery of dead patients within his heart. Those deep ventricles are a Davy Jones locker full of dark secrets and trauma. The agonising calculus of squeezing maximum benefit for no harm has always proven to be impossible. No matter how hard one tries to do good, very bad things, on occasion, happen.
Only if one has ever been in that wretched position, will one understand. One is left with a patient dead body and one’s own stripped of its soul. Hero Complex, at once, becomes Absolute Zero Complex.
One might wake at midnight and see the dead patient’s death in one’s eyes, or in the bleary eyes of a mirror, toothbrush in mouth. In one’s dreams, on the street, in the supermarket. One sees it in the eyes of every patient who smiles, takes ones hand and gives thanks for one being the greatest, kindest doctor ever, the only one whoever listened and helped. If only they knew. It remains forever unbearable.
There are some special medical environments where we might further forgive noble but fatal errors of judgement and genuine, unavoidable complications. Those environments are typically in theatres of war, or in impoverished countries where there is chaos, poor system and little resource.
What remains unforgivable is the meticulous method with which chaos, poor system and little resource was wilfully created and imposed in the West. All for a common cold, which was proven very early on in the faux pandemic propaganda to be just that by the Diamond Princess study.
Even those professionally trained to kill are forever changed and traumatised by it. Somehow, the systematic, mass killers are immune to the grief of it.
Officials such as Matt Hancock and Antony Fauci must have cemeteries of hundreds of thousands of bodies trapped inside their blotted chests. The deep guilt of having one body’s blood inadvertently on one’s hands is intolerable; how much more might theirs be? How much more atonement and redemption for their sins? Why do their hearts not also burst with the pain?
In 1976 it took 12 deaths to pull a vaccine off the market. Now, millions can die & be injured from a vaccine & people seem numb to it because of propaganda, fear & lies
Conclusion
This book, necessarily written in adversity with risk to its team, is truly an extraordinarily calm, and scientific exercise in medical understatement. It is an utter damnation of modified mRNA gene therapy. It offers chilling, woefully unique and rare insight into a global crime scene. No wonder it is ignored by those who profit from it. Those who are extremely powerful and wield an increasingly centralised digital wand which imposes tyranny, mesmerises masses and manipulates reality. We are persuasively killed by State cures and soothed by the salve of State lies. This little red book is the indelible evidence of their multiple homicides.
It is because of Prof, Burkhardt and his team’s courageous scholarship these poor slaughtered souls have been given powerful voices from beyond their premature graves.
This book is a stained histopathological, photographic history of the stinking truth of the covid crime and it deserves so much more attention and accolade. It should be mandatory reading for all doctors. It a quiet, reserved but shining exposé. The likelihood is it is already victim to an internet misinformation vortex viciously vacuuming truth, reason and morality from our world.
Buy a copy and lend it to your misinformed doctors, this Christmas.
28th November 2025
Please let me know in the comments about your own, related experiences. Please share this with your doctor, and let me know the response.
All links are archived and if broken may, in the majority, be found by searching the link on archive.isor, in the small minority, on web.archive.org
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, asprescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
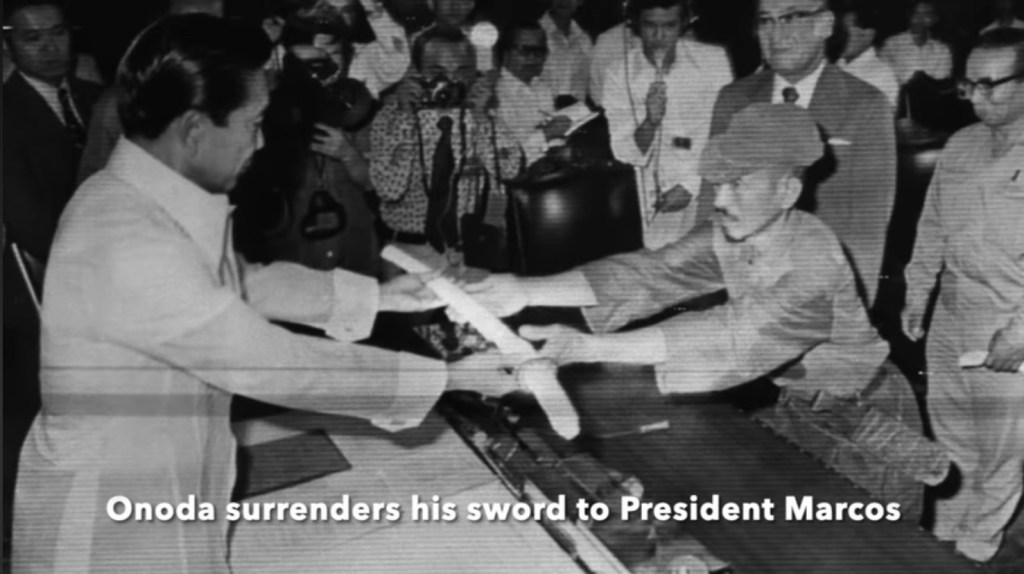
Perennially Entrenched: 2nd Lieutenant Hiroo Onoda surrendered in 1974, an astounding 29 years after the end of WWII
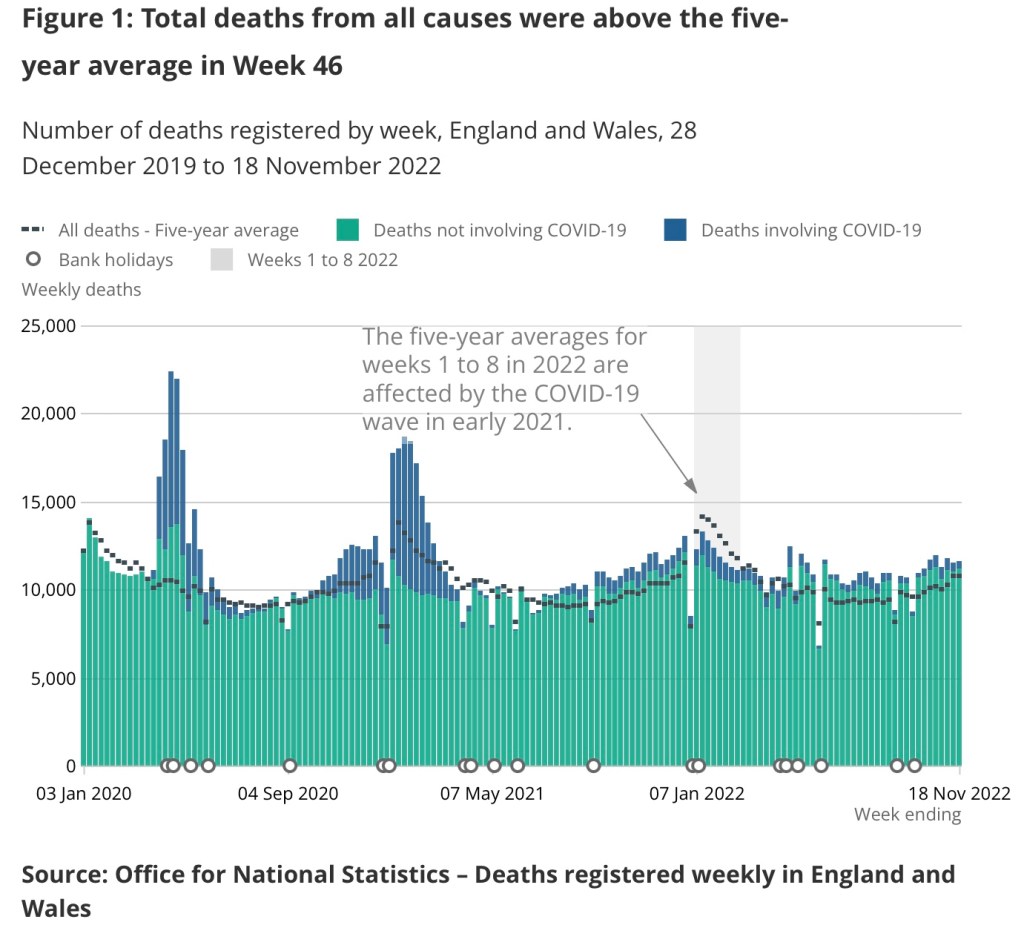
Another interim despatch from the mundane, microcosmic, rump end of COVID-19: The Greatest Show On Earth. It indicates that potential adverse effects of the current rounds of JCVI and government-recommended covid jabs continue to be felt in our communities and go unacknowledged by our authorities and the mainstream. It continues to prove that as sure as sheep are sheep, so are most of us.
I continue living covid, still livid at covid: the jabs, a ritual mass poisoning. Long after VIC, Victory in Covid Day went at once unannounced, presumed, denied and claimed. All whilst covid (the pandemic bit) never happened. The conspiracy of jabs for profit and control remains hard to criminally prove, and the admission of damage and guilt politically unacceptable. These competing narratives remain lingering around me, after former colleagues have fled the profession prematurely, moved on in denial, or sold their souls more deeply.
This August was the 80th anniversary of VJ-Day, Victory Over Japan. The majority of Japan’s armed forces surrendered on 15th August 1945, but many small groups and individuals did not. Incredibly, the last recorded Japanese only surrendered in 1974, a mere 29 years after the end of WWII. Such entrenched behaviour reminds of the many colleagues and patients still bunkered down, in late summer 2025:
A late-summer flurry of positive tests, 2025
Mrs Banzai!
Autoimmune 55 year woman on an injectable immunosuppressant for a rheumatological condition, presenting with a very sore throat and temperature. Just tested positive for COVID-19 in the month August 2025. True to form, as an identikit child of peak commie-fascism, her priority is an ‘antiviral’ i.e. PaxlovidTM, or potentially even some kind of intravenous concoction of immunoglobulin.
These existential questions continue cropping up. Had she not tested positive, she would have perhaps remembered her priority was my priority: check the white cell count. The real threat was potential neutropenic bacterial tonsillitis. The real action: stop the methotrexate, start antibiotics.
Unfortunately, her five-year prevailing view was, ‘I will die of covid,’ because she is one of the patients who is made to feel perpetually clinical extremely vulnerable by the scriptwriters in Whitehall. Had she not tested positive for covid, I am sure she would not have thought, ‘I have flu, I need an antiviral, lest I die.’
Such cod narrative makes the doctor clinically extremely vulnerable, too. Fortunately, the digital formulary would not even give me the option of prescribing PaxlovidTM, and so I very gladly packed her off to A&E for someone else to do the damage to her, if she so wanted it. Before doing so, I explained that her condition’s priority, in my opinion, was not an antiviral. It never has been with most so-called viral infections. Covid has transformed the narrative. Patients and doctors now believe that just as antibiotic is to bacteria, antiviral maybe to virus.
Master Kamikaze-Parent, 17
Teenager with psychological issues. Actually, issues I suspect caused by Covid lockdown policy in school, and certain parental proclivities.
The parent wants antivirals for the son, for he has gluten intolerance which in the parent’s artificial intelligence-groomed mind means he has an autoimmune condition. To her, in turn, this means he is clinically extremely vulnerable. It is gobsmacking.
The family all have mere colds, and all test covid-positive. This, the parent uses as a reasonable argument against false-positives. I slip into her narrative. I beg to counter with the fact the original pandemic wasn’t at all dangerous to most, particularly not to children. Further, the government had conceded the pandemic was long over and therefore did not need to be associated with mass panic. It had reassured us the ‘variants’ were now even less serious than they actually were in the first place.
The paradox of her continued pandemic fear in 2025 despite the whole family being covid jabbed remains an unmentionable. This is the banality of abnormal health within the political incantation of the new normal. Again, I shield behind my inability to prescribe what the parent thinks the child needs. So it’s, listen to me or go to A&E. Listening to me wins, but, I believe, only because the hospital is too far away.
I would suggest the fact the family is all jabbed is exactly why it is all unseasonably feverish with a flu-like illness in the hot summer of 2025. The mother of that then 14-year-old child took her to have her two or three covid jabs – she can’t quite remember how many, just as she can’t quite make a link between them and their current malady.
Ms Chesty Cough, 55. A breath of fresh air.
Finally, that day, a middle-aged lady. Just returned from abroad, never jabbed, has done a covid test. It returned positive. With baited breath and trepidation I called her – what would such an clinical non sequitur possibly want? What she did want ought to be the final pragmatic epitaph to COVID-19: ‘Doctor, just returned from abroad, never jabbed, developed a chest cough and did a covid test which returned positive, just want some antibiotics, please.’ That it was not PaxlovidTM warmed my heart.
1974: Onoda surrenders his Pfizer to President Marcos
The Spring-Summer 2025 Covid Collection
The UK spring 2025 covid-jab campaign had presented its own particular revival of post-jab disease. The patterns are temporal, and so similar in clinical presentation as to, again, strongly imply not only a correlation but a causation. I submit yellow cards, I record my concerns, and I insert concern where I can when the patient is not too demented or liable to take offence (with a “what do you think this pattern might be telling you?”) and then I try move on, unflustered.
It is early May 2025, and we are at the end of about round 10 of the covid boosters. That thing which was only needed twice, safe, effective and that was all, the scamdemic having allegedly finally finished in summer 2022. Spring 2025 augurs another unseasonable wave of chest infections, hospital admissions, and frivolous hospital antiviral prescriptions. Add to that the new normal of weird covid jab-related pathology. Most seem to be in their seventies or over, and therefore prime, continued targets for their governments. Does it represent the cumulative burden of trusting obedience?
My consultation room has become a confession chamber for those elders:
Never, again, I am fed up.
Doctor, why are they still doing it?
More pertinently, why did you, and why do many of you continue to accept them?
Some geriatrics remain the obedient serfs of the landed gentry. No amount of capitalist hyper-individualisation and indoctrinated hyper-sexualisation with the freedom to copulate like juveniles on cruise liners in the Mediterranean has taught them to think critically, have faith or to self-respect.
Mr Barnacle Biceps, Late septuagenarian
Possible skin carcinoma, clinging like a large, ancient ocean barnacle to his lateral biceps, surrounded by hyper-melanotic macules. He says it only started soon after he had the initial covid jab in the exact site of its injection. He says it pointedly and with, I feel, an inappropriate relish, tapping at it, ‘EGGx-actly There, Doctor.’ He thought it would detach when bored and leap back overboard. It did not. For 4 years it has carried on growing, and growing. He is referred to the skin cancer clinic.
Intrigued, I follow the case like a limpet. The additional irony of it is he is seen by a distant plastic surgeon, online via a grainy, rural internet connection. My virtual colleague does not even see what I referred the man for. He focuses on the equally-concerning macules, and making short shrift, dismisses them outright. I wonder if the patient has the nous to realise the barnacle in the room may have miraculously dodged the digital data stream. I move on in a professional frenzy. What can one expect working in a system with a safety net like an abyss? In the NHS we trust.
Mr Heart-Failed Octogenarian
An intelligent man whom I saw in late April this year. A minor chest infection. Treated simply and efficiently with a penicillin. 10 days later he is much better, and unbeknown to me, he is invited to see a modern Florence Nightingale for his spring covid jab. As most his age, he is on about number 10.
He reasonably asks whether it is wise as he is not quite over the chest infection. Florence shoves a thermometer in his ear and pronounces, ‘apyrexial, computer says jab’. This is stupid, since, fevers swing.
That night, his heart packs in. Acute biventricular, congestive heart failure. He is rushed to hospital. He nearly dies. His elderly wife, left alone to manage the fall-out, falls at home and nearly dies in the turmoil of his sudden post-jab turn for the worst.
He only had one serum troponin, which was on the rise. No one in the hospital bothers to do a second. So we will never know if heart failure was induced by a myocardial infarction or myocarditis.
On his ward there is an ostensible influenza outbreak (this is mid-spring). These things didn’t happen like this before the jabs. The reaction is indiscriminately veterinarian. It is to dope everyone on the elderly ward with antivirals. As a consequence (the consultant’s view, not mine), my patient now lapses into renal failure. Still only semi-recovered from the combined traumae of community and hospital healthcare, he is palmed off to the outpatient heart failure nurse. She is similarly algorithmic in her care, ratcheting up the obligatory ACE-inhibitor which does his straining kidneys no favours.
It is a month down the line from me nearly successfully treating this man when I realise after communing lengthily with a computer screen that the rest of the NHS has been misdiagnosing, mistreating and nearly killing him. He looks at me, a shadow, with brain reeling from hypoxia. I am shaking my head in disbelief as I catch up with his exciting month. It is so bad, if it weren’t real, it would be a special kind of hilarious. Black humour hilarious. The kind which makes the ribs and the loins hurt badly. But, it is true. It is also a lot to digest and process in a ten minute appointment.
It is an exhibition par excellence of how to fell a man in several, algorithmic pharmaceutical steps. All without engaging a brain cell. There is no nuance, no rational.
Too many (systemically-blinded) cooks spoil the broth
I turn to him and suggest he must decide if he wants me or the heart failure nurse to manage him. I know I am no longer master of my manor. There are many, new less experienced squires on the plural pastures of mechanised medicine. He looks at me without any deliberation and nominates me. I am almost flattered, but it was, for most of my career, my professional privilege to lead patient care until covid came.
Heart failure nurse nearly has a heart attack. She claims there is conflicting advice. There wasn’t really. She was treating past numbers and applying non-holistic, rigid protocol. I was individually treating the current patient, holistically. I commit no crime. The compliance-algorithm nurse is very angry. She says to the patient she will speak to my junior doctor colleague – the ‘clinical lead’- whom, she was sure, would, quote, ‘fall into line’. As always does she. I have become the problem, since, I think, analyse and question in the best interests of patients. Thus, I am no longer welcome in general practice. It has become an extremist cult of medicalism. No evidence, no experience, only obedience required. A health system for hacks, managers and their superiors, not for doctors, nor even patients.
At this point no one in the NHS is properly engaging the brains which were systematically disengaged by relentless government and media covid propaganda. They follow orders, leaving a buried trail of preventable suffering and death behind them. There is an additional queer NHS phenomenon. In their letters and to patients, my hospital colleagues invariably do not enquire into nor acknowledge the clear temporal relations of the covid jab to the pathology, even if I expressly mention it to them in my referrals. In doing so, they are complicit in forever-rendering the concern impertinent and invisible.
Pemphigus or Pemphigoid: three leaky patients
Mr Bubble Wrap, 80
Early spring 2025, I’m sent to a local care home to see a man with multiple unexplained blisters. Relapsing, remitting and migrating all over his body in a seemingly random sequence. Mmmh, Pemphigus or Pemphigoid? Odd. I begin the usual experiments with various topical and then oral treatments, scratching my head, finally ending in oral steroids as usual last resort. They work temporarily, but as soon as they are removed, out crop the blisters, again. He is put on a metaphorical slow boat to China in search of a dermatologist.
I return 4 weeks later for a seemingly unrelated matter and realise the close, unusual connection between the 10th covid jab instalment and a second patient in the same nursing home.
Mrs Blister Pack, 89
She is the second post 10th jab pemphigoid occurring in the same nursing home, with the jab having been given by the same oblivious nurse, on the same day. This patient had been managed in parallel by a colleague, siloed from my independent observations – both eventually fail to resolve with standard diagnoses and treatments. It leaves the vax as a culprit.
There’s no use climbing the walls about it anymore. Nothing happened at the start. Nothing will happen now. There is every likelihood the observant, on-point doctor announcing a correlation will again be treated like a criminal or a front running candidate for a lunatic asylum.
Yellow card ADRs are, as usual, recorded by me. But, nothing has changed. Nothing will. There was enough concern to pull the jabs before rollout, and more after jabs 1 and 2. We’re on jab 10, and it has long become a lobotomised, continuing assault on the old, uninformed, and vulnerable.
Mrs Bullous Pemphigoid Jr, The Third, 83
A third patient with the leaky dermis. She is an earlier precedent, who comes 6 weeks after, and confirms my hunches on the other two leakers. A dermatologist-diagnosed case of bullous pemphigoid, after the first two jabs. She has been on on a constant trickle of oral steroids since 2022.
The greater tragedy is that she is continuing to have each and every jab offered up to her. I mention very innocently the pattern of dermal leakiness I have noticed. The attendant daughter, not that shocked, takes the hint and seems, with her body language, to indicate things might be different next time. I ask her to give my regards to her mother’s dermatologist.
Leaked truths
Finally, as it used to be pre-2020 and before the scandalous propaganda of the MHRA. Professional Life mirrors clinical research. At last, there are cracks appearing in the dam of lies erected against research leaking truths, published in an academic paper:
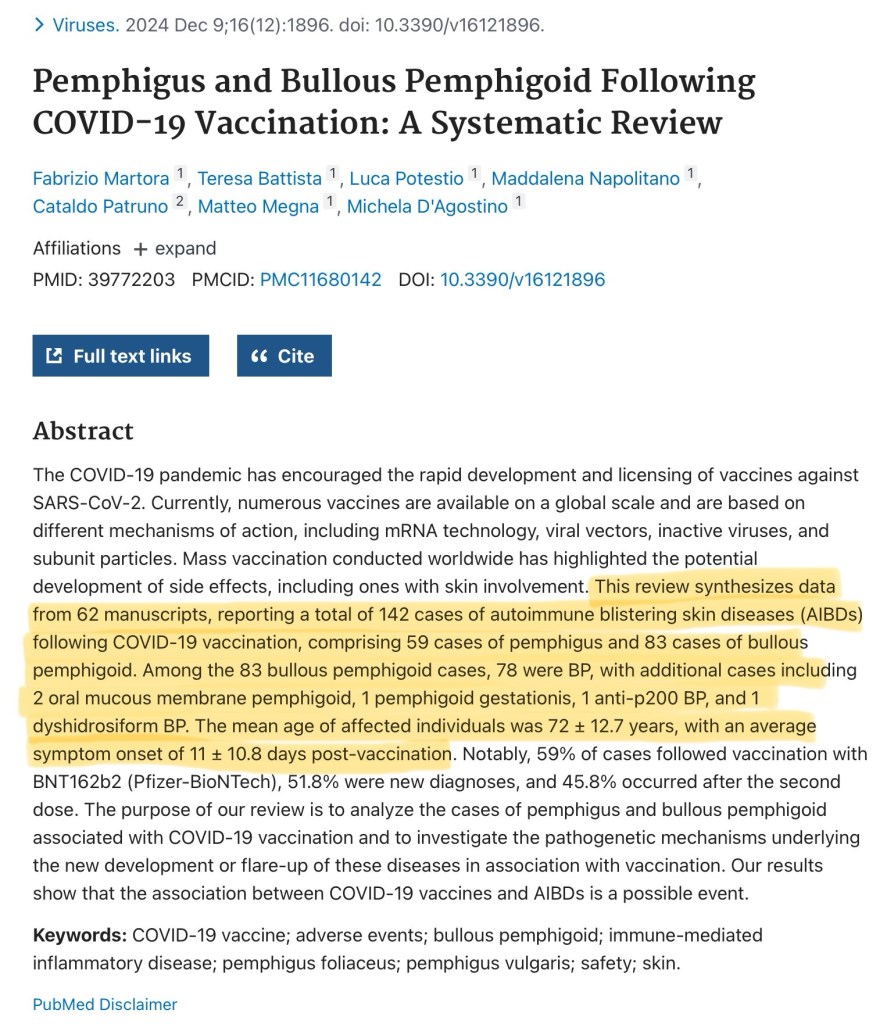
“Pemphigus and Bullous Pemphigoid Following COVID-19 Vaccination: A Systematic Review: This review synthesises data from 62 manuscripts, reporting a total of 142 cases of autoimmune blistering skin diseases (AIBDs) following COVID-19 vaccination, comprising 59 cases of pemphigus and 83 cases of bullous pemphigoid. Among the 83 bullous pemphigoid cases, 78 were BP, with additional cases including 2 oral mucous membrane pemphigoid, 1 pemphigoid gestationis, 1 anti-p200 BP, and 1 dyshidrosiform BP. The mean age of affected”
The Creaky Carer, 60
This 60 year old care home worker, had 2 jabs under State duress of destitution, and now embodies late-onset inflammatory arthritis and a lifetime anchored to expensive blockbuster biologic injections. She dares to say, ‘may I ask if it could be the covid jabs?’ because most likely, she has heard I am even open to very reasonable questions. I affirm her question. By running through the research and my own clinical experience, I absolve myself of professional quackery.
There are many of these demographic autoimmune disease anomalies since covid injections. Untimely, unusual, unnecessary. But not now unexpected. Sadly, the rheumatologists in hospitals act like it is normal. Never once taking a recent jab history, never once questioning the new abnormal. They must be seeing more concentrated series of abnormalities than me. I am subversive, the patient is questioning. I suggest when she sees the expert to ask the obvious, unmentionable question on all sufferers’ lips: could it be the jab?
Young Farmer Angina, 43
A non-smoker, a wife and two young children. In the end I have to admit however unlikely it used to be, this formerly very active, physically fit man may have severe angina. Rapid Access Chest Pain Clinic, here we come. He regrets having the first three jabs and he loathes the government for, after destroying the medical profession through covid, destroying farmers through taxation. In any case, he is no longer fit enough to run his own farm. The State are belt and bracing his destruction.
This 2025 pre-print on, ‘The intracellular aggregation of encoded spike monomers and their subunits as a cause of cardiac side effects’ states:
‘The arrangement of these complexes always adhered to a consistent pattern in each cell type. Particularly in AC16 cardiomyocytes, the various spike protein derivatives impaired not only cell proliferation, but also induced a pro-inflammatory response and oxidative stress.’
Ms Croaky, 75
An acute dysphonia and pyrexia two days post-jab – is it a coincidental laryngitis, or is it something else? Could it be post-covid jab ?(herpetic) recurrent laryngeal nerve palsy? These days it is all on the cards.
Mr Another Seventy-something
Another seventy something. Five days post-jab in the left deltoid, he develops symptoms of an ipsilateral arm, brachial plexitis. Oh well, we’ll just have to see what happens… what else is there to do?
In-the-know Farmer’s Wife, 77
Farmer’s wife is asking after her delayed replacement hip operation. A hip well-worn proving a life well-lived. Hip aside, and as if to mitigate her one weakness, and without being led, she spontaneously says she has been as ‘Fit as a fiddle in the last 5 years, and I’ve not had one of those jabs … I know what’s in them’. Actually, I’m sure that she does not, but I know what she means. She appears as a rare apparition sent by the universe to fortify me in a lonely plight.
Mrs Unseasonal Pneumonia, 76
It is late spring, 2025. She nonchalantly has 10th jab. I comment equally nonchalantly at the un-seasonality of Mrs Unseasonal’s pneumonia. Breaking into what is altogether an uncharacteristic u-turn, she cocks her head professorially, ‘I have noticed that in other people. I ONLY got chest infections at winter before.’ However, she carried on jabbing, being the trooper she is.
‘I guess you have to balance the risks,’ I say charitably; and in concession, ‘they do peddle it by saying you could be worse without it.’ Before biting, ‘But, some of us have not had one and not been ill in 5 years.’ Says I, who has been on the faux frontline of nothing in particular, facing these coughing, spluttering, covid PCR positive masses.
Mr Chesty Nonagenarian
On the same day, a 93 year old man, with a similar ruttle, since a week or so after a COVID booster in the residential home. Chesty, and breathless. I sardonically point out and underline the close correlation to the attending care staff, who already know this correlates. The covid jab seems at once a slow-kill, fast kill method, all locked in by fear of a worse death, or of reprisals.
Mr Chesty is too demented to take the hint, so he will progress to the 11th booster level and by then we will again be at the gates of winter, and he will have to contend with the combination of the triple-whammy: jabs of flu, covid and the winter. This may well be the mortal blow. The irony that he may have jab-induced dementia is not lost. The research data on spike protein-induced neurological damage continues to accrue, as in this paper, but, true to the wilful blindness we have become accustomed to in tyranny, not once do the researchers dare mention damage-potential via injected spike protein gene templates.
potential genotoxic, and therefore neoplastic risks of bio-engineered viral spike protein. These academic rascals cannot allow themselves to inevitably extend their conclusion towards the bio-engineered spike protein gene vaccines.
Mrs Ever-Thinning, 75
Mid-June 2025, retired, widowed, fading away for about 18 months to 2 years, weight dropping, total serum protein falling. Body scan shows no cancer. Bloods, essentially otherwise unremarkable. After the tenth covid booster, she collapses, and receives seven stitches to the forehead. The shocking blood pressure of 80/40 is deemed ‘her baseline’ by A&E. Contradicting the emergency doctor’s narrative of convenience is the action of 250ml of intravenous fluid bolus to resuscitate her before a CT scan.
She is sent home with a low serum potassium of 3.2 and hypotensive. Barely able to lie back in her bed. A concerned district nurse calls me in, her standing systolic blood pressure is 67. I ask if she felt unwell after the covid booster? No, she replies. Yet, 48 hours later she did collapse.
The CT scan demonstrates some ground glass opacities in the chest, with a plan to repeat the scan in three months. That is all. After this gross incompetence, is it worth or is it safe sending her back? Lord knows. I try again to point out the obvious in a hurriedly scribbled letter to my colleagues and hope for the best as I call another ambulance.
She is skeletal, slowly, indefinably and non-specifically wasting away. No one can work out why there is a non-specific slow change in one lung base, she is too weak for a bronchoscopy. Yet, she dutifully has every covid booster. One wonders what could have been had she not. We will never know. We are where we are. She feels they are safe, effective and necessary – but for whom?
I want to tell her to stop, but I know she is so locked in and so obedient to the State, in the way only a lifer in the teaching profession might be. She would consider the very suggestion a call to death, not life. At best, it would confuse, anger and distress her. So, the death spiral continues spiralling.
Mrs Relatively Frank-Clot, 83
She had a pulmonary embolism after the her fifth and final jab. She is on permanent anti-coagulation. She stopped having jabs. In a remarkable and rare moment of clarity, she reports she was told by her hospital doctor, ‘They could not rule out a link.’ This is more honesty from a doctor than most have received.
‘The consistent subclinical changes in inflammatory and coagulation markers suggest that these pathways may be involved in the pathogenesis of severe ARFIs [sic] (adverse events following immunization) reported with mRNA vaccines.’
Mr Another-Weird Post-Jab Rash, 81
He is sent an SMS call to covid arms. He dutifully answers it. Two weeks post-10th covid booster, he develops an atypical evolving, migratory generalised inflamed, itchy red discoid rash to his upper back, the left upper arm and right lateral calf; there is a danger at the leg and upper arm of the skin eroding and becoming infected. I turn up the steroids, and note the developing patient series of post covid jab dermatological pathology.
Ms Secondarily Infertile, 29
Two times Pfizer in mid-2021. Never returned for the third because her periods stopped somewhere between the 1st and 2nd jabs, and for over a year. Eventually they returned, then she miscarried. She is desperate for a child. Her leaders are desperate for her to not. Her pregnancy is officially unsustainable. The young couple have, since, been unable to conceive for two years. Time has made her candid. Today, she says she believes it was the jabs. Professional experience tells me this is reasonable. What else is more likely?
‘Successful conception rates were substantially lower for women vaccinated against COVID-19 before successful conception than for those who were not vaccinated.’
Little Miss Arthritic, 18
Three years of paediatric joint issues. On examination, an acute-on-chronic polyarthritis with raised of CRP 57 and a rheumatoid factor of 39. She cannot recall if she had any vaccines around the time of onset. Yet, she did, in October 2021. When reminded, she cannot recall any issues with it. Yet, for some reason, even unbeknown to her, she did not complete the course of two. She does not seem to care. She, instead and without basis nor correlation in time, wonders if a hormonal implant 8 weeks ago has anything to do with the 3 year illness.
Celtic Mother Earth Figure, 54
She is feeling fatigued these days. She arrives, with big hopes. She wants to be tested for every vitamin and mineral known to man. She’s there to fine tune her health to perfection. I drop it gently that there’s no way the NHS will provide all that, but I’ll do what I can. Such was her interest in perfect health, that, as she stands to leave I ask, in fascination, ‘did you have any of the covid vaccines?’
She stops, her face drops, her shoulders round and she hunches her back and almost dissembles, ‘Unfortunately I had three. I wish I’d never had any… but I didn’t know then… and I’d had a bad flu… and I have a (minor) chest condition.’ It seems she had rehearsed her excuses very well, but, there was the concealed, deep regret many now have. I commiserate her, ‘Some people are still having them, on number 10 or 11.’ We bid farewell. I have a queasy suspicion she led her little girl down the same path.
Five and a half years later, in spite of desperate continuing and current attempts to resuscitate COVID-19 pandemics, there was and is no justification for giving unnecessary, unsafe and ineffective jabs.
“IRREFUTABLE Grounds for Immediate Market Withdrawal of COVID-19 mRNA Injections,”
“Together, the international evidence has converged: mRNA injections are unsafe, ineffective, contaminated, and in violation of international law,”
McCullough et al continue to add to the ever-increasing pile of indictment ignored by institutional blindness and wilful obfuscation.
The crime of covid jabbing continues to be perpetrated by casual, normalised NHS hands which themselves would now, never wish to receive in kind. The continuing crime scene is now geriatric, mainly confined to care homes, the demented, and institutionally-ignorant. Also, those extremely scared of death and dying but nonetheless not of iatrogenic illness and death. Then, in contrast, there are the journeymen patients who take the multiple jabs like a well-worn punchbag, they neither seem to flourish nor perish. It is also true to say, that I have countless more patients who by being unwell call into question the jabs. My current enumeration of cases is not by any means exhaustive.
Newsflash
In the last week of August, a message flashes up on the screen. A colleague leading the charge in the old people’s homes:
[BANZAI!] Warning, 9 residents just tested positive for COVID.
I couldn’t care less. What does that mean? Does it mean they are unwell? Does it mean testing is meaningless? Does it mean the ongoing jab campaign is not only dangerous but futile?
I shrug and carry on. It is a continuing human folly I want no part of. To me the implied disaster is unlikely, in a hot summer, and there has been a trend this season for patients and carers to start testing again. There is no real disaster on the ground apart from the population being more unwell than before the jabs, with strange disease outbreaks following each round of jabs. The less jabs, the less disease. I do wish they would stop it.
So, what actually is ‘covid’? It is an excuse of quickly transforming the relationship of the State to the individual into a tyranny in order to implement whatever change the controllers of the States wish.
Will we ever emerge from World War III?
Epilogue – A Brief Encounter
Dr Confessional Purgatory, FRCGP, late 50s
GP appraisal, late 2025. A process ushered in by a serial killer colleague. Intended to prevent sociopathic killers entering the profession. It doesn’t. It helps hide them. For, the exercise is one of decerebrated regulatory compliance. One witnessed the dark place this precise, obedient attitude dragged the profession during covid.
My appraiser, a very senior colleague, perhaps in her late 50s, provides a sad end to the proceedings. The process has been abstracted into an on-line platform because of covid, and remained there. Over three years, I have been incrementally stretching her tolerance with allusions to covidology. Each year she has smiled benignly, and once even dared ask my covid vaccination status. My reply was a polite, Foxtrot Oscar.
This year, she emails last-minute: Not enough evidence of CPD (continuing professional development) to pass go. I have plenty of evidence, but it is all taboo. I determine to let rip. I apprised her of recent research discussing dermatological and cognitive disease potentially caused by ‘covid gene immunotherapy injections’. In my portfolio, I dispense with the use of the vernacular ‘jab’, but cannot bring myself even in this confessional torture chamber call them ‘vaccines’.
Last year, I had gently alluded to cardiac, thromboembolic and cancer concerns. Today, I am prepared to be severely challenged over stretching her dogma to the limits. I am taken aback by the response:
She says, You know, you go into things in such depth. I have a learned a lot from you in the last three years. I will miss our meetings… I’ve had heart problems in the last two years and now I have a pacemaker and it’s not really relieving my symptoms of fatigue properly. My blood pressure drops and I feel terrible but they tell me everything is fine. And my partner, well he’s young and he’s developed cancer in the last two years, and it’s only since he’s had these jabs…had chemotherapy… and he’s so frightened, he keeps having the covid boosters. He’s on number 10. And… you know, funny you should mention it… his memory… his memory isn’t as good as it used to be… me and my son, he’s also a GP, we’re wondering whether it’s a good or bad thing.
She mentions that there was a young doctor at the practice where she is a partner who refused to have any of the covid vaccinations, as if it was somehow abnormal. It was, clearly, not absurd. I reply, ‘that seems to be a sensible response given it used to take 10 or 15 years to develop a vaccine, and that, allegedly, this one took six to eight months.’ I mention that one of my relatives is a pharmaceutical chemist and works in the regulatory aspects of gene therapy, to back the statement up.
It’s our last of three years of appraisals, and my appraiser bids a slightly emotional farewell. She looks more tired than at the start, having forcibly been slid into semi-retirement by ill health. Slim, but sarcopenic; receded, impossibly-dyed hair line and a droplet-belly belying a weak core. It is a tragic picture. Frankly, she looks knackered.
She says, ‘Well, I’ve learned a lot from you. It’s been an education.’
Has it?
You’re an unusual person? You are… ummmh… errr… eccentric.’
‘Let me help you. What you’re trying to say is I am abnormal.’
‘Yes, actually. Perhaps you’ve got something like ADHD or Asperger’s… you go into so much… detail.’
Her statements speaks volumes about the profession, where it is, and why it cannot change direction. It is medicalising, and therefore making abnormal the quality of basic competence. It is defeated, unwell and confused.
She continues to ramble, ‘My partner, we’re not sure what he should do about upcoming (11th) covid vaccine… but I think I’ll have the flu jab and I think he will, too.’ They remain trapped between a rock and a hard belief. Could she not see the pattern for herself in her privileged daily position in front of her damaged patients? My patients could.
I almost cannot contain my astonishment, ‘Well whatever you do, don’t have both together on the same day,’ and I, jaw now suitably loosened by her candidness, reiterate the horror of what happened in my practice, Christmas 2022.
She looks helpless, confused and trapped. I try help her out, ‘Well, I’m not really sure what’s going on but it’s a really difficult position when the State says one thing and your patient and you know a different thing… I guess we’re all prisoners of our own Truths.’
‘Yes, yes,’ she nods fervently. She again mentions that she has learned so much from me in the last three years. This continues to shock me, as we both accept that a misfit like me would never be allowed to be a leader in our profession of medicine. She has been extraordinarily helpful and kind over three years as my appraiser, sensing that I was different, from the off.
Finally, Like a scene from a Brief Encounter. There is a rapid gushing of yet, unrequited words. A quick transfer of ‘turbo cancer, SV40, DNA contamination, Angus Dalgleish’, and a final turn of heads in the night, amidst the steam and whistle, to frantically wave and shout, ‘Use Yandex, or you’ll get Google-Nowhere!’ It is The End of The Affair.
This is the frank, urgent interchange between medical colleagues that should have occurred everywhere, five years ago. Yet the profession is still siloed in the comfortably dumb bunkers of medical normalcy. For me, these medics may have been so deeply entrenched in a superficial denial of in-the-face facts, they put short-term individual survival in front of long-term collective benefit.
For five years, a minority of doctors and patients have privately been meeting to whisper, some individually publicly screaming in pain and being correspondingly severely punished. Sometimes they have written and published, secretly, for the best interests of everyone. They have been roundly berated for consistently being proven, in real terms, correct. Our brethren have remained in the trenches, as major opposition. Finally, they begin to openly ponder surrender, of coming up for air, of raising white flag and daring to admit self-harm, of aiding and abetting the harm of others.
15.9.25McCullough et al: “This sentinel case report [healthy 31 year female] provides the first documented evidence of genomic integration of mRNA vaccine-derived genetic material in a human subject, documenting a temporal association between COVID-19 mRNA vaccination and aggressive malignancy, reproducible multi-omic evidence of oncogenic signaling, and a non–safe harbor host–vector integration event.” Source & Preprint
1.9.25Bread and circuses:Doublespeak from Warp-speed POTUS Mr. DJ Maverick Flip-Flop Puppet. Do not hold your breath. We are due a SPARS pandemic. Source: X
”One of Britain’s most eminent oncologists, Prof Angus Dalgleish, said for me to share with you today that he thinks it’s highly likely that the Covid vaccines have been a factor, a significant factor, in the cancer of members of the Royal family.”
3.9.2025 Surgeon General Dr. Joseph Ladapo Announced That Florida is Ending Mandates for ALL Vaccines, “Every last one is wrong … Who am I, or anyone else, to tell you what you should put in your body? Who am I to tell you what your child should put in their body?” Indeed.
8.9.25The United Confusional States of America:Trump’s recent thimerosal remarks will be used to promote the alternative, poisonous modified mRNA injections, and may not at all achieve redress for the dead and damaged.
Please let me know in the comments about your own, related experiences. Please share this with your doctor, and let me know the response.
19th September 2025
All links are archived and if broken may, in the majority, be found by searching the link onarchive.isor, in the small minority, onweb.archive.org.
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, asprescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
Recent research slowly emerges to suggest covid jabs are associated with chronic neurological illness and cognitive impairment. This is being reflected in clinical practice.
A recent Friday. Another extraordinary day in the collapsing edifice of Medicine. In my case, in doctor-led General Practice. Today was gravid with tragedy meeting full circle. Within five years, the serpent head of Asclepius has coiled into swallowing its own rattling tail, whole.
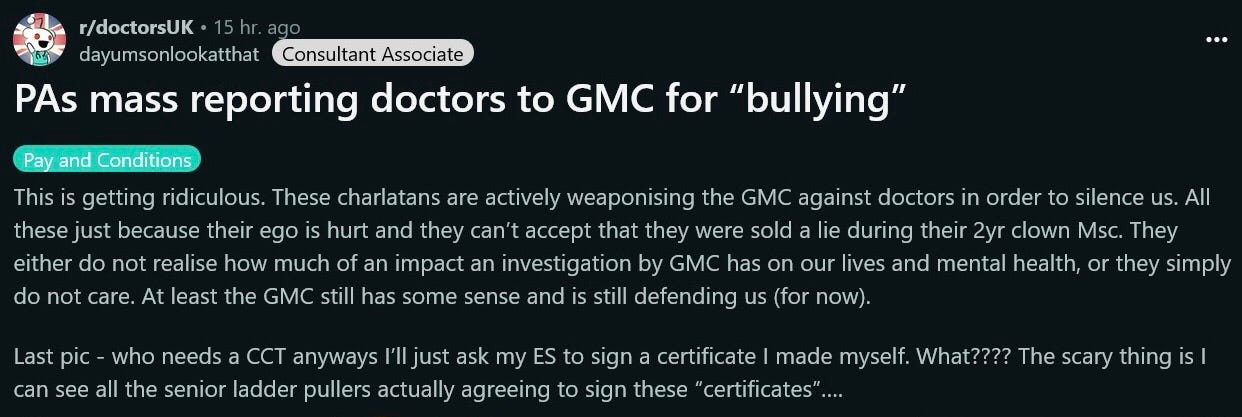
Perhaps, the fall was spiked in the name. General and Practice. For, nearly all and sundry are now permitted to generally practice pharmaceutical poisoning at the sacrificial altar of the GMC and NHS. The GMC is no longer only for doctors and, no longer holds any of its menagerie of regulated individuals to proper ethical standards.
In my last article I wrote of observing an unusual but definite trend amongst some elderly couples attending consultations together. One a decrepit patient, the other the supportive, ageing spouse. Neither remembering the details of why they were consulting me. Pre-covid, the usual presentation was a demented male with a compos mentis female spouse pre-destined to post-decease him. Some readers have asked me to elaborate.
Much, but still not enough, has been made of the more apparent acute jab sequelae of cardiac events, strokes, large clots, died-suddenly in peak athletic condition, and fatalities within close temporal proximity to jabbing.
Slow-burning morbidity and mortality slip more easily under the clinical radar. Who in the system would even wish to notice, when the Pharma-enabling MHRA connived with the nursing and medical professions to inadequately consent the masses into unnecessary, dangerous, and experimental (ostensibly) gene injections masquerading as ‘vaccines’. It is more easily arguable these injectables (and not a putative SARS-CoV-2) were bioweapons more than they were vaccines.
Before elaborating on covid jabs, one must also acknowledge the real contribution of enduring mental and cognitive damage caused by tyrannic covid policy upon many (now, hyper-neurotic) young and (now, very disorientated) elderly people. Of course, the UK has an increasingly ageing population that in itself is associated with neurodegeneration, but even so, there is a whiff of something else in the air.
In the past, I have alluded to unusual post-jab presentations of narcolepsy and motor neurone disease. A quick review of recent academic literature shows a reluctant admitting to of very concerning neurological safety signals, with reference to the covid injections. It confirms the heightening clinical suspicions I have harboured in my own small clinical sphere for many months.
Bouncing Baby
The week before, an emergency admission of an irritable, hypertonic, puce-faced two month old with the most prominently-bulging anterior fontanelle I’d ever seen. My fingers bounce on it, palpating repeatedly in disbelief. Feverish. Less than a week before it had the hexavalent DTaP/IPV/Hib/HepB vaccine (why do all newborns now require routine protection from a blood and sexually transmitted hepatitis once the preserve of intravenous drug users and health workers?). The stunned mother palmed the infant to me with an anergia of rejection. It felt as if she was already detaching from it in preparation for the worst.
I admitted baby with: (?)post-vaccination meningitis. A few days later, after a shot of ceftriaxone, it was sent home with the lazy and perfidious diagnosis of ‘viral illness’. No paediatrician worth their registration is capable of questioning vaccines. Will autism be this child’s fate? No doubt the mother will submit the child to more of the same booster vaccines. Come what may.
Ms Confined by Fibromyalgia, 60
I involuntarily forewent breakfast as the proprietor of my usual eatery could not get out of bed. Fibromyalgia. For her it is a diagnosis of affirmative honour. For me it is an expanding, syndromic basket case. A basket case which attracts basket cases. Not that most are not genuinely afflicted by some thing. Many cases may be iatrogenic, vaccine-injured and basket-misattributed, or environmental toxin in origin. But, allopathy lacks the ability, will and the honesty to understand and admit to these.
She has only developed debilitation in the last five years. Like many others. To her credit she stopped at three jabs and does not without good warrant long for Long-Covid.
Ever-expanding Fibromyalgia Syndrome has had mission creep over the decades. Once it was pseudo-nuanced by discrete, symmetrical tender points. Now it is not. It maybe that the creep is professionally functional. It gives rheumatologists a way out from admitting ignorance without appearing ignorant.
There is change in the air, today. My alternative newsfeed is spooning me a mainstream news diet. Daily Mail:more vaccine damage revelations, 5 years after the revelations. There’s more post-fact Daily Mail facts: Long-Covid may be P.V.S, post-vaccination syndrome! Except covid jabs are not vaccines, not even when the WHO and CDC tried to capriciously redefine them to fool the world into a death-trap.
T.D.S
Aside from FMS and PVS, there is TDS. Trump Derangement Syndrome. Trump is still trumping. Trumping everywhere and everyone. Again, withdrawing the USA from the WHO, along with a few more nations, this time. If ever, to paraphrase the apocryphal quote of Native Americans, Orange man spoke with forked tongue, it is Trump. Compare his 2025 rhetoric on Palestine and Ukraine. Compare his beautiful vaccines with M.A.H.A. Is this more 5D chess from the Grandmaster? Let us see what he does rather than heed what he says.
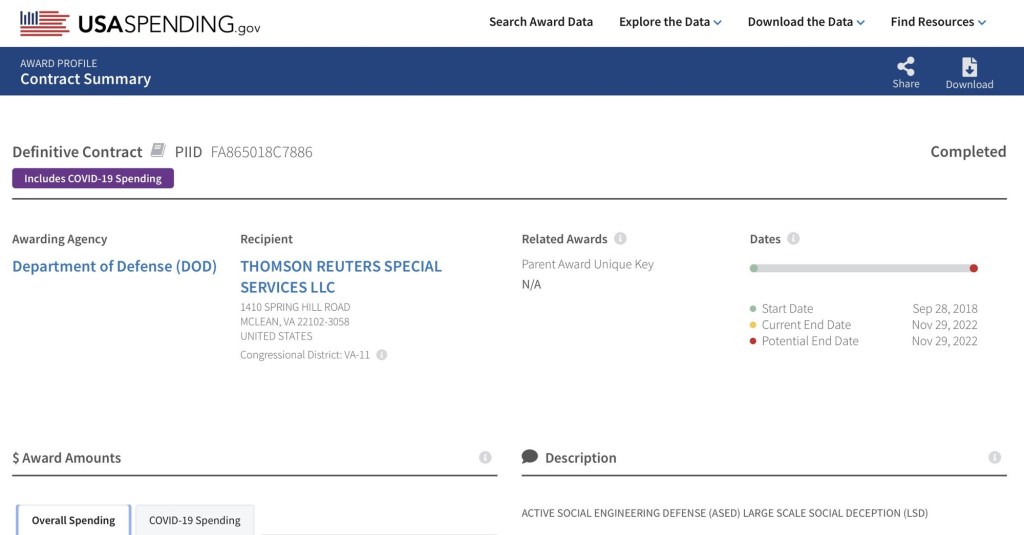
Since 2019 one has been brainwashed by the USA into thinking a US military countermeasure was a necessary, safe and effective by USAID funded Reuters fact-checking propaganda. See bottom right: “Active social engineering defense (ASED) Large Scale Social Deception (LSD!)” (Source: X)
The morning gets worse, despite 30 minutes gained by foregoing breakfast:
Mrs Does Not Remember Wobbling, 74
The first patient is a pleasant and retired lady. As if armed with the permissive Daily Mail scoops, she arrives pronouncing, as now are many: It all began with the booster. Three days after the covid booster she knew something was wrong. Severe chest pain and Richter Scale generalised rigors. However, they got better so she carried on being injected. Five years later, the jaw has loosened. It may now be safe to talk without retribution from an NHS doctor. She has chosen the right one. In 2020, blue-rinsers such as she would have shopped this doctor into the police state.
The fascinating problem with the consultation is she does not remember why she booked the appointment, not even when prompted by me. She believes it was to talk about a minor blood test. The fact she booked the appointment originally for the reason that ever since starting serial covid jabs she cannot ambulate properly and is progressively worsening is now not important to her.
Not even when I share a discussion with her I had with a colleague about one of their patients:
Dr Hands-in-Pockets, 74
That patient is 74 years old. An eminent older physician, still working. Someone who swallowed the jabs whole, and someone who would bite a colleague’s head off if one had warned him of the dangers. Even he is slowly becoming open to the suggestion something is wrong with the jabs. Why? Because, since the serial jabs he can only walk forward if he leans back his torso, plants his hands in his pockets, and then cocks both elbows back. At least he is reasonably cognitively intact.
My amnesic, early-morning patient has double trouble. Extraordinarily, she describes exactly the same bizarre motor disorder, with a similar way of overcoming it to achieve forward propulsion. Two instances in a week of something never before described to me.
However, she cannot remember why she came, and therefore cannot remember why I would be recounting a similar patient. She brings me back to the reason why she thinks she came, butDoctor, it’saboutmy blood test. She protests when I say the consultation time is long over. She tells me I must not be able to understand her, that it is my fault. It is not. It is the State’s fault. This whole sordid mess.
It is impossible to meaningfully and civilly process this clinical complexity in ten minutes, with or without the obstructive propaganda of the State. I frantically dive in to her notes to try make amends. The system allows me no allotted time to read clinical records before seeing a patient. It turns out the issue of the blood test had been dealt with weeks before she saw me.
Even so, I offer her another slot with a colleague to appease her, on the same day. I even warn my colleague, Go easy, I think she has cognitive decline. We need to address it. He nods, in scholarly comprehension. I check her second consultation of that same day. Short and sweet. She wanted to sort her already sorted blood tests out. That is all my colleague recorded. Will she complain? I doubt she will remember.
Headless Headmaster, 80
The second patient is a retired headmaster, with all the dignity that brings. 80 years. It started in 2021 with ‘ever since I had covid I haven’t been right’. It is ending in 2025 with ‘ever since I had the covid jabs I haven’t been right’. The narrative shift is timely, and I believe, correct.
He continues, TATT (tired all the time) and brain fog. Has to stop walking in order to rest after every few yards. Had the booster jab and felt a weakness and numbness soon after, travel up from tips of toes to the waist. Could have had (overlooked) post-vaccine G.B.S. (Guillain Barré Syndrome). I commiserate. Lucky he did not end up on a ventilator for GBS. Did he mention it at the time to any one in healthcare? No. Why not? I guess, as with many others, the impenetrable lie of ‘safe and effective’ and necessary kept him mute and on-side with the thought police.
No longer. Oh, no. He continues to spill the beans. He had the flu and covid jabs on the same day, Christmas 2024 and felt awful. Oh, how he shook!Never again would he suffer in complicit silence. Except, obedience for short-term survival at the expense of long-term incarceration is a personality trait which sticks. I have learned only a few of us have an ingrained absence of self-preservation that prioritises the importance of truth over currency and calories.
Again, he has cognitively declined since covid. He won’t accept it. Again, it causes intra-consultation conflict. How does one preserve the peace in an impossible ten minute consultation? What is certain is that the pressure of NHS practice has aided and abetted the damaging lie of covid.
Perhaps, I should ignore the obvious, pat his back and platitude him out of the doorway. But it feels wrong. I delve into his notes and we find his cognitive score has objectively fallen from moderate to severe in 18 months. He concedes. His daughter keeps pointing out his failing memory. Where he rejected my referral to memory clinic in 2023, he now accepts a referral to the memory clinic, 2025. Later that month, he will decide to decline it, again.
Memory Clinic
Memory clinic may preserve, or produce some practical cognitive improvement for a few through Big Pharma blockbuster pro-cholinergics. What it will never do is implicate vaccines, gene therapy or statins in dementia. The thought that lowering cholesterol through statins might be the first cause of the Western pandemic of dementia seems reasoning too far for mainstream medicine. According to DeepSeek AI, 25% of a human’s natural and essential cholesterol resides in 2% of the body’s mass, the brain. It insulates brain wiring.
The NHS memory clinic does serve a useful purpose. It scans the brains of these demented patients. Increasingly in these covid times, I am seeing more microvascular and mixed dementia being diagnosed rather than Alzheimer’s. These other varieties often do not meet the criteria for the so-called memory drugs.
I would hazard a guess that were one to biopsy these post-covid brains, there may be evidence of non-Alzheimer, spike protein deposition and neuro-inflammatory pathology. Regrettably, the potentially neurodegenerative covid jabs were targeted to those with, and most vulnerable to neurodegeneration. Professor Burkhardt was a pioneer in recommending a post-jab post-mortem protocol. His work may form a basis for truthful answers.
It is easy to see why jabs may be neuro-pathogenic. A serially-injected, modified mRNA gene therapy packaged in a blood-brain barrier penetrating LNP shell, its DNA contaminates, the consequential perpetual protein machine, and all the pro-carcinogenic and pro-inflammatory adjuvants are a recipe for mixed dementia and brain cancer. Yet, this concoction is still being recommended and given by States, globally. There are only now suggestions with RFK Jr’s M.A.H.A. mandate we may at least see some temporary pause to the madness.
Academic Research
With reference to a potential jab-induced, persistently neuropathological gloop, a study, according to the CHD, says this:
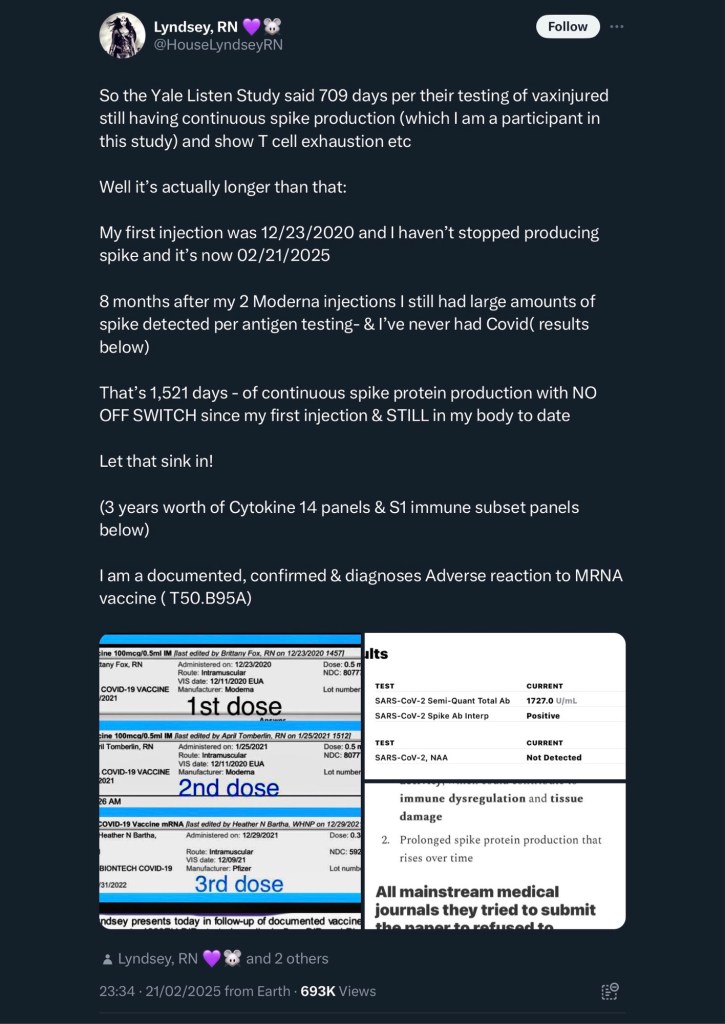
Yale University researchers found that people thought to be experiencing long COVID may be suffering from post-vaccination syndrome. Researchers detected the spike protein in the blood of vaccinated study participants from between 26 days up to, in one case, 709 days after vaccination.
Covid-19 jabs: perpetual, toxic Spike protein machines (Source: X)
A 2023 review of neurological side effects of COVID-19 vaccination says:
The most important and common complications are cerebrovascular disorders including cerebral venous sinus thrombosis, transient ischemic attack, intracerebral hemorrhage, ischemic stroke, and demyelinating disorders including transverse myelitis, first manifestation of MS, and neuromyelitis optica.
In 2024, the mainstream of academic medicine is asking the diametrically wrong-question, and dejectedly concluding:
The relationship between COVID-19 infection and a possible increased likelihood of older adults developing new-onset dementia (NOD) remains elusive.
At the same time some in academia are asking the pertinent, correct question. This 2024 paper concludes:
Preliminary evidence suggests a potential link between COVID-19 vaccination, particularly mRNA vaccines, and increased incidences of AD (Alzheimer’s) and MCI (Mild Cognitive Impairment). This warrants the need for further research to elucidate the relationship between vaccine-induced immune responses and neurodegenerative processes, advocating for continuous monitoring and investigation into the vaccines’ long-term neurological impacts.
There is a fascinating pre-clinical sign of dementia. Anosmia. Loss of sense of smell. I will quote Wikipedia. It may inadvertently provide a lead on a link between the covid/covid jab narrative and increasing dementia:
Sensory dysfunction is claimed for the pre-clinical stage, which may precede the first clinical signs of dementia by up to ten years.[11] Most notably the sense of smell is lost,[11][44] associated with depression and a loss of appetite leading to poor nutrition.[45] It is suggested that this dysfunction may come about because the olfactory epithelium is exposed to the environment, and the lack of blood–brain barrier protection allows toxic elements to enter and cause damage to the chemosensory networks.[11]
One only wishes careers had not been destroyed when people such as my anonymous self concluded the existence of such unnecessary real risks in 2020. Even Pfizer admitted to them in February 2021. Yet here in 2025 they are still highly recommended for the most vulnerable to them.
Regional Revelations
Perhaps, I have misapprehended the extraordinary clinical trends I am experiencing professionally, or maybe they do not generalise more widely. However, my experiential deductions have not been wrong about covid since 2019. Will we ever have due, candid discussions and studies of these phenomena?
Sadly, at a time of increased need, my locality’s neurology service has collapsed. For some reason it cannot employ a neurologist. Probably due to defunding and a government which broke us all financing the businesses of covid and endless war.
Perhaps, covid-jab neuropathology increased our neurologists’ distressing workloads; or maybe the curated unwillingness to honestly discuss the contribution of covid jabs to their impossible workload demoralised the incumbent neurologists to the point where they all fled?
In the pre-artificial intelligence age, abandoned nurses are being entrusted to manage the neurological complexity post-covid jabs that GPs refer to absent and over-stretched hospital neurologists. In the same way, State psychiatry has gradually, and for longer been whittled down toward an eventual technician-led endpoint. What this health service demise can be sure of producing is the situation where no one left in neurology will be brave or qualified enough to speak out against the jab’s mythical reputation.
I share my woes in the reception room, What an extraordinarily dismal and depressing day. A senior nurse, no doubt reined into herself taking and then giving covid jabs to our population, makes an extraordinarily open statement: I think they are trying to kill old people.
This NHS thought crime is not met by any disapprobation from any of the co-conspirators present. How ever brave the statement made on NHS property is, it does strike me as not being quite on point. There remains a cognitive dissonance in this professional day of broken covid narratives. I reply, but we have been given this stuff to children, too. Silence. I walk away.
Et tu, Prof. Swaying, 88
Later, at the weekend, I visit a senior colleague. A legendary old lecturer from medical school. 88 years. Wife died ‘of/with covid’ 2020. Hence, no questioning of the covid narrative can be had, and furthermore, he must be terrified of dying ‘of covid’. Still jogging until 18 months ago, but now feeling decidedly unbalanced.
Mercifully his excellent, precision memory does not need jogging. The cardiologists are discussing more pacing wires for re-emerged atrial fibrillation (and there has been an awful lot of that post-jabs). We stand, discussing the diagnosis. He stands lean, learned and tall. Hands in pockets, elbows pinned back, swaying at the waist. My diagnostic subconscious mind is pondering as we speak. (?)Post-serial covid jab (?)truncal ataxia? The possibilities are brain-boggling. I cannot divulge to him. He is old school. Medicine remains to his retired and excellent mind a noble profession. Each to his fate.
Dr Roger Hodkinson FRCPC, FCAP, Oxbridge, Biotech innovator. He deserves due credit as a heroic early defender of medical reason & ethics. In 2020, he gave a blistering admonishment of covid tyranny to local authorities in a viral conference call at the Community & Public Services Committee, Council Chambers, Alberta, Canada. In 2024, he like many was targeted by regulators. (Source: X)
Dr. Clotted Brain, 57
The week was ingloriously capped by other major clinical colleague news. I discovered a dear colleague in her mid-50s, with retirement in touching distance is unwell. She was already adequately anti-coagulated for unrelated health reasons. Even so, she suffered a major thrombotic CVA. Life and function saved by a thrombectomy.
She had a winter 2024 covid jab booster, for perceived other vulnerabilities, two weeks prior to said stroke. Whether she will have another jab depends on the balance of fear and propaganda rather than any in-born intelligence and useful medical experience. Even she has become just another victim in the ritual normalisation of the giving of unsafe, unnecessary and ineffective pharmaceuticals.
Pfizer, MAHA & Trump: Lunacy or Buxom Multi-dimensional Chess-mastery. Crowd boo Bourla. Trump shuts them up. Trump was a confirmed pill-taking proponent of Professor Didier Raoult’s hydroxychloroquine for Covid-19 advice. See his 19.3.20 White House briefing.
Finally, at the end of another Friday of chaos in the crumpling NHS, more revelation. Another alternative drop from a Telegram account: Trump lauds Pfizer CEO and Fascistic Veterinarian, Dr Albert Bourla. Crowd boo Bourla. Trump shuts them up. 5D Chess-master at work or 44DDD chest posturing?
It was a fast moving week, and an even faster-moving Friday. Certainly, bringing into question the covid jabs is no longer quite the revolutionary act it used to be. 2025 feels as if it might be different, maybe.
Please let me know in the comments about your own, related experiences.
27th March 2025
All links are archived and if broken may, in the majority, be found by searching the link onarchive.isor, in the small minority, onweb.archive.org.
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, asprescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
Disunited Kingdom of Dystopia, Winter 2024. The Pandemic’ was officially declared ‘over’ May 2023
Preface
“ACCORDING to the testimony of all ages, no occupation is more unanimously declared to be a conjectural art than medicine; consequently none has less right to refuse a searching enquiry as to whether it is well founded than it, on which man’s health, his most precious possession on earth, depends.
…
The results of my convictions are set forth in this book. It remains to be seen whether physicians, who mean to act honestly by their conscience and by their fellow-creatures, will continue to stick to the pernicious tissue of conjectures and caprice, or can open their eyes to the salutary truth.”
I suffered the recent ignominy of being shoved out of the doctor’s car parking space. My crime was arriving for work fractionally earlier than a colleague. A shout across vehicle, dripping in thick regional accent, ‘Can ya move ya car? I’m coming an’ a going, today. I’ve gorra do all the spring covid visits.’ My colleague was doing the rounds in the elderly care homes. It made me shudder and scuttle away. The colleague’s medicine had only the proven utility of earning money. In 2024, even Joe Bloggs knows such conduct is insane. Where are the mass-propagandised notions of ‘no pandemic’, ‘unconscionable risk’, and ‘natural immunity’ when they do not support the off-loading of the dangerous, unnecessary and unscrutinised pharmaceutical products of government contracts?
Pharmaceutical-Grade Military Censors
Could US intelligence service have really conspired with free speech censorship and international public health law, to propagate serial injections of gene technology into every man, woman, baby and child on the planet, under the false premise of a serious respiratory virus pandemic? Genuine academic, scientific and medical opinion, and research continues to convincingly maintain it did. The only pandemic of global seriousness by these analyses was that of merciless State propaganda, misinformation and a vicious censorship of reality. It was a pre-programmed, lockstep event with the intent of massive profit and the direct effect of loss of liberty, mass delusion and global iatrogenesis. The sophistication of which is matched by the scale of continued State denial of an open secret.
In the UK, there was combat level narrative control by our own military against us. Clearly, the most dangerous group to the 77th Brigade were doctors and scientists who know better than the State and the general population. Therefore, professionals and experts dissenting from the propaganda had to be aggressively persecuted, censored and removed from the equation of population perception management.
Big Tech recognises its overwhelming control over the global population consensus. Reality is either censored by, ‘Not on our corporate platform’, ‘hate speech’, ‘subjectively offensive’, or ‘misinformation’. At the best, an erratic lip-service to freedom of expression sometime prevails by shadow-banning, at the expense of a freedom of visibility of expression. In entirety, it amounts to unreasonable censorship of a healthy consensus on reality. In its place, Big Lies are laid, led by elite arrogance, armed with a compass of sociopathic immorality and engineered wokeness funded by our taxation. We pay for our cage.
Those with open, inquiring, libertarian minds are left unwelcome, ultimately financially and digitally cancelled under the tide of a technocratic tyranny. How is it that humanity and society can sink so low? It is inevitable when profit is put before merit. Why did the elite allow Covid to happen, when every real, factual imperative indicated the implausible covid narrative was disproportionate, dangerous and destructive to health, humanity and the Western democratic status quo? Perhaps, because it was.
“This provision [21 USC 360bbb-3(k)] and the entire structure of the EUA Countermeasures law uncovered by Katherine revealed how the US Government systematically removed all consumer safeguards for the products designated as military “countermeasures” under contrived, arbitrary, self-proclaimed conditions of “public health emergency”, and then lied to the public pretending that these were properly approved safe and effective pharmaceuticals.”
“Her writing provided the critical piece of the puzzle I was looking for: it explained how the criminal cartel, including actors in the US government, military, and private companies “legalized” and implemented the covid atrocity.”
The push to write publicly in summer 2020 was inspired by others. By John Iaonnidis et al (March 2020), Dr Zev Zelenko (March 2020), Professor Didier Raoult (April 2020), by Dr Mohammed Adil’s early, prescient criticism (11th May 2020) of government delusional propaganda. Dr Adil has now been struck from the UK medical register. By Attorney, Dr. Reiner Fuellmich’s pivotal and barn-storming video statement of spring 2020. Sadly, Dr. Feullmich is becoming the Assange of Covid having been imprisoned, without conviction. He has been on remand since 13 October 2023 and in isolation since 10 June 2024. By fellow GP, Dr Malcolm Kendrick (26th June 2020). At the time, his was the only other early public criticism I knew of covid policy by a working UK GP. Dr Claire Craig (9th September 2020), Dr Mike Yeadon (20th September 2020) and Dr Tess Lawrie (December 2020) and her group, British Ivermectin Recommendation Development (BiRD) Panel which directed me toward further potential but suppressed generic therapies. All were officially vilified. All corroborated with my serious and quietly held real-life clinical concerns and observations.
My covid perspective, was of a holistic, working UK family physician, armed with real time, incoming medical data, access to hospital death notifications and the responsibility of writing certificates for deaths in the community. There was no way I could not know what was truly happening and not happening. If one also understood basic medical science, basic medical statistical method and the basis of the PCR tests the pandemic was predicated on, one was left professionally chilled by what worldwide governments were saying and not saying in unison. The online Worldometer kept winding up the PCR positive test-associated death toll like the US national debt.
My first essay of October 2020 amongst their solitary voices was another watershed moment for simple, honest, concern. It was inspired not by courage but out of an existential necessity. Until then, and even now, I have not seen such a continuous, frank professional chronicle representative of the mind of an ethical, covid-questioning medical doctor in practice during the extraordinary propaganda of the global covid regime.
I realised I had an unusual professional vantage point from where to integrate the various counter-narrative ideas. I saw no pandemic. I saw damage temporally related to covid gene technology and denial of access to healthcare, employment and the freedom to survive, wherever I worked in the world. Chilling does not come close to describing the feeling of the disconnect between what I knew, and what I did and did not see when compared with what the government impressed upon my patients.
Unsurprisingly, those colleagues who spoke out tended to be retired, or already struck-off from medical registers. Those who were still working and did the same were fired, disciplined and continue to be struck-off. I knew enough of life to know this would be my fate. Thus, I began to diary, and then publish my truth, anonymously. It was my moral, ethical and professional duty to do so in the face of my patients being misinformed by those whom they are indoctrinated to trust. Thankfully, some heard me and were armed with useful information on which to make informed choices during covid.
I am grateful to those who published my early essays, and to the various platforms that re-published them. Certainly, by November 2020, Truth in the Timeline of Covid became ‘viral’ in a regime of extreme Ofcom and GMC censorship. It was, in its own way, a stone in a catapult to fight Goliath, when in 2020 only a handful of scientists and medics were speaking out. I can report that the tide is turning with grass-root patients. Many now see The Lie. Between words and consultations a healthy understanding can be achieved, whether the State likes it or not.
I began warning of the madness of the covid jab even before it appeared and was rolled out. Time has vindicated me. I do not believe any of my main concerns and points have been proven to be wrong by the passage of time. I wish they had. Even though my first essay seemed prescient to my naïve mind, it was not to the already-initiated such as Professor Sucharit Bhakdi and Dr Wolfgang Wodarg.
Mine was a story of a doctor attempting to give as many people the benefit of my clinical observations in real-time as the lockdown policies and covid gene therapies were irresponsibly disseminated. I had to balance this against the risk of being professionally destroyed by regulator over-reach. I considered I had an ethical duty to speak out while still remaining present for my patients, and to make known my simple, honest clinical observations at the heart of the NHS for posterity. My professional thoughts seemed to resonate with others’ secret concerns, contrary to a narrative that was intended by the State to be unquestionably, and unimpeachably perfect. This was the first red flag. Science and medicine never are. Dogma and cults are, always.
What struck me about the responses to me daring to voice my truth was how few doctors commented or followed suit, and conversely, also, how many laypeople did seem to come up for air, and commented with gratitude for some sort of doctor coming out to finally confirm what they felt in their bones but which was rendered unconscionable by the State.
17th December 2024, Australia. The reinstated victorious Dr William Bay, hero and victim of State persecution. He is a channel for many medical doctors. Meanwhile, 17th December 2024, UK, Dr Daniel Armstrong is struck off. If the comments below this article are representative of the public, the regulator of public confidence in the medical profession has itself lost public confidence. General Medical Council, or General Mission Creep? Reinstate all such doctors.
I saw the covid narrative change from a postulated, severe, rampant killer respiratory syndrome, typified by ARDS secondary to microvascular pathology, with improbable R numbers and fatality rates. By January 2020, covid imperceptibly transmuted into an asymptomatic, non-fatal, non-specific phenomenon typified by no particular clinical symptom, sign, pathology, nor specific treatment. It was the perfect pretend Petri dish for EUA, CMA and MEGA-PROFIT. The diagnosis of this nondescript entity was misattributed to human, animal and inanimate objects by a flawed, false positive PCR testing procedure. The cause, said to be a virus, never seen at the scene of the diagnosis, never fundamentally in itself proven to materially exist or actually be harmful, but always presumed to be there and responsible via unreliable surrogate markers. Yet, it was said to be easily and consistently apprehended by homemade face cloths, and tamed at mealtimes in restaurants. A criminal court could not convict with such bad framing of a suspect. A criminal court could not convict with such bad framing of a suspect.
The disproportionate draconian response to the hysteria remained commensurate to the urban myth and corporate profit. Individual professional clinical autonomy, and patient bodily autonomy was illegally outlawed by States. An unproven, improperly tested, toxic gene therapy was mandated. This enforced, unnecessary, global human experimental assault, intentionally or unintentionally, created a massive pandemic of fatal microvascular, macro-vascular, inflammatory and immunologically-driven pathologies the like of which the world had never seen.
Most medics transformed into unethical, obtuse State instruments, overnight, neglecting their professional duties. Imagine if fire fighters refused to attend house fires out of fear or government advice, and instead, danced; or soldiers the frontline. Nurses and medics were found in dereliction of their sacred duties. Somehow, the professions and the public accepted this. It was truly a delusional moment, where greedy, corrupted and incompetent government actors and narcissists rapidly indoctrinated their incorrect assertions and beliefs into the minds of public and professionals, alike.
Governments, public servants, scientists and healthcare workers sold inevitably unsafe injections with fear, but made adoption look cool, collective and compulsory. Even if, somewhere inside, they knew it was scam, shame-worthy to humanity, and dangerous to their own kith and kin. They strained the meaning of law and words until they meant the diametrically opposite, or nothing whatsoever at all. Until medical practice equated to a total political obedience to government and regulator.
The covid over-reaction viewed in the context of the geopolitical situation seems like a simple lever to threaten and coerce individuals and countries into sacrificing sovereignties, utilising the WHO and its tyrannical globalist constitution, the IHR, as a fulcrum. It can be no mere coincidence that soon as covid leverage was dropped as the global population cosh, Russophobia replaced it. No coincidence that China was funded and legislated by the USA to engage in gain-of-function experiments with coronaviruses, and Israel expands through Syria Palaestina toward Damascus. No mere coincidence that Pfizer held to ransom South American nation for toxic ‘vaccines’ in exchange for military bases as financial and legal collateral. There is a 2030 timetable to this globalist project and the implementers of it appear unwilling to wait.
Could it be that China was set up as the fall guy, with unlikely images of Chinese falling like timber in streets; that other focused chemical, radiation or bioweapons, rogue or not, created large clusters of ill health, and the rest of the pandemic was propped up by a wilful PCR test-demic, statistical manipulation and propaganda? China Virus, hydroxychloroquine, warp speed and Regeneron became Trump memes, and all while Chinese scientists wrote scientific papers enabling the WHO to frame an in silico culprit. Are all nations, by definition, mere patsies in the great game of conglomerate globalism? It is mind-boggling. That is the point of psychological operations. One’s head boggles more if the false pretext on which this mother of all psy-ops occurred happens to be one’s professional domain.
Apart from skullduggery, one must further contend with the possibility that not only traditional, flawed academic mathematical modelling was used in hyping the fear, but also that novel, amoral A.I. algorithms and data synthesis were employed by State entities in making extraordinarily unusual decisions to break from traditional pandemic wisdom. Wilful misattribution and disproportionate, fatal over-reaction fomented by an impulse for greed, control and a now, recurring political mantra of, to save you from death, we must end life. Never again must the world be duped by commercial and political tyrants.
The most clearcut and dangerous global pandemics of 2020 onwards were caused by the government-propagated lockdowns on life, and by the pharmaceutically-synthesised and healthcare system-injected, replicating toxin. The irony that a modern vaccine should be a toxic man-made virion is missed by most of the world.
Revolution after Convid?
We should be allowed to make our own choices and our own mistakes, untainted by overwhelming State misinformation. The problem in the phenomenon of covid is only the shackled mind of the covid cult was afforded liberty. Covidiots such as myself were not allowed even to be seen to be right. It is an unfortunate fact that many mass movements which think they share broad libertarian and human values selfishly deny that equal right of freedom, informed consent and bodily autonomy to others when confronted by the selfish urge to protect and pursue their own narrow agendas. Such is human nature towards others’ natural human freedoms.
Even now, the increasingly damning data, there from the start, is being ignored. One can be plucked out from 8 billion and persecuted endlessly but the State cannot transparently reveal copious research, excess mortality and morbidity data. Medical colleagues exist simultaneously in improbably parallel worlds where patients were dropping dead, coagulating, haemorrhaging, and miscarrying prematurely in unprecedented numbers, where the hyper-coagulating AZ jab was suicided from under their very noses, and ‘Long Covid’.
Yet, still they are to believe these Covid jabs are unimpeachably safe and effective. Read of consultant cardiologist, Dr Aseem Malhotra’s personal and professional torment by covid policy’s implementers and his evidenced stance against covid shots, here. Does it seem like Medical McCarthyism, yet? Malhotra is being pursued by anonymous doctors through the GMC and High Court, determined not to allow him have a contrary and equal right to free professional expression. Why the professional anonymity? It is not as if they are the victimised, oppressed minority.
It is becoming increasingly apparent in my medical practice that patients are more than ever, preternaturally and otherwise, falling prey to ischaemic heart disease, atherosclerotic, and thromboembolic disease, and falling prey to it again, and again. I have premature arrhythmias, CABGs, stents, re-stents, strokes, cancer, and dementias, notably including more vascular dementia, coming out of my patients’ ears. Married couples in their sixties arrive together, neither able to properly remember the details of why they are here to see me. It is unprecedented. Have prescriptions of dementia, anticoagulant and arrhythmia medications risen? We are compartmentalised from realising these trends. Covid has taught this is how the State clearly likes it to be. Again, my concerns continue to be vindicated by hushed official Pfizer reportage, with latest Pfizer leaks suggesting heart conditions in the covid jabbed worsening over time.
Often, medics make clinical medical and surgical decisions based on consensus dictated by the prevailing general medical culture, regional culture, or by time-honoured practices. Sometimes even on the science alone. In covid, the tested culture of respiratory infection and pandemic management was mutilated by enormous State propaganda and corporate interest; and the relevant scientific and epidemiological data was hidden, redacted or distorted. Clinical reality was ignored and confirmatory clinical tests were abused.
It is remarkable how my early, simple clinical observations, safety and ethical concerns were corroborated and continue to be by a tapestry of various academic research, figures from science and medicine, patients and their families. We have all independently and reluctantly had to come to the same, sane conclusion by different means that the official covid narrative continues to be wrong, and the covid gene therapy unnecessary, dangerous and ineffective. The remaining question is, was the death and global damage intentional? Was covid driven by greed, power and cover-up, alone? Or was it a conscious attempt to cull the human population and spirit?
Ultimately, a centralised world is a world at the total mercy of singular algorithmic tyranny. It is a world where national and bodily sovereignties are merely a globalist’s tools reinforced and undermined with equal brutality. Reinforced by supra-nationals to justify coerced conscription into certain damage and death with a misplaced, suicidal Nationalism. Equally undermined by the WHO to justify coerced global conscription into certain damage and death by covid gene injections. A tyranny which is pro-life when it is pro-profit and anti-health, and pro-killing when pre-natal and pre-death. The tyranny institutionalises perpetual conflict where perpetual cooperation is more easily attainable.
There is certainly something very wrong with the vaccination and virus narrative in the context of vaccines for viruses. When the State categorically states they are necessary, safe and effective, we now know categorically they are not. So, the State and the official science is specious and not to be trusted. A virology that it is based on shadows cast by surrogate markers presumed to be from a virus is not a science to be applied.
The science and medicine around disease thought to caused by viruses remains often speculative, damaging and ineffective. Take Bell’s palsy or shingles variously treated depending on the prevailing fashion with anti-virals, steroids or nothing at all, with similar outcomes. Both pathologies are now also ostensibly both caused and/or treated by anti-viral vaccines. Take cancer, once desperately wished by the CDC to be viral in aetiology, but now arguably also caused by anti-viral covid shots. Take HIV and AIDS, once treated with fatal anti-cancer chemotherapies, now with anti-retrovirals, while controversy continues as to what causes, and what actually is AIDS. Take T-VEC, ostensibly a modified herpes virus, being trialled to treat melanoma.
The more one probes, the more one feels virus vaccinology and catastrophic respiratory pandemics are misused as fables of convenience for the general population, by fear-mongering profiteers and control freaks.
A Frank Physician
Saturday June 20th 1942, “After May 1940 the good times were few and far between: first there was the war, then the capitulation and then the arrival of the Germans, which is when the trouble started for the Jews. Our freedom was severely restricted by a series of anti-Jewish decrees: Jews were required to wear a yellow star; Jews were required to turn in their bicycles; Jews were forbidden to use streetcars; Jews were forbidden to ride in cars, even their own; Jews were required to do their shopping between 3 and 5 P.M.; Jews were required to frequent only Jewish-owned barbershops and beauty parlours; Jews were forbidden to be out on the streets between 8 P.M. and 6 A.M.; Jews were forbidden to go to theatres, movies or any other forms of entertainment; Jews were forbidden to use swimming pools, tennis courts, hockey fields or any other athletic fields; Jews were forbidden to go rowing; Jews were forbidden to take part in any athletic activity in public; Jews were forbidden to sit in their gardens or those of their friends after 8 P.M.; Jews were forbidden to visit Christians in their homes; Jews were required to attend Jewish schools, etc[…]”
Excerpt from, The Diary of a Young Girl, by Anne Frank
Picture a frank doctor suddenly trapped, hiding in a bio-fascist home country, with genocide being policed and implemented by her colleagues. The only thing she could safely too was secretly document it in her unpracticed style. This was me.
Replace war with pandemic, capitulation with Lockdown, German with Globalist tyrants and Jew with The Unvaccinated and The Locked-Down. Now, change the year to 2020. One has Covid. Jews were unforgivably mistreated as if they were infested or infestations, with the collusion of the German medical establishment. Those of us who did not bow to mandated toxins were also unforgivably and particularly mistreated, with the collusion of the global medical establishment. When the blitzkrieg reached France, my colleague’s un-jabbed daughter, out studying there for the year, was not even allowed in a shop to buy bread without showing a current negative PCR test. We had our means to subsist stolen. We were denigrated, denied and destroyed with the threat of unemployment, relocation and death.
Even the yellow star had a yellow sticker covid analogue. Those who wished to be allowed remaining human liberties had to sacrifice fundamental bodily freedom and comply with the bioweapon shot (it has been coherently defined as one by a legal scholar of them). Many of those were criminally maimed and died. Nobody cared. No authority will properly acknowledge it. We need it acknowledged. We need to draw parallels. We, too, need our voice, unbridled by affected outrage. Jewish news site, Forward, featured Anne Frank-covid comparisons, 6th April 2020.
Defamation and Mass-Killing
During the covid tyranny I learned about moral relativism, intersectionality and divide et impera. That politicians are the frontline workers of ignorance. About the weapon of subjective offence as a major sop in our conception of justice. One editor I encountered would not allow a comparison of Nazi instigated suppression and genocide with that of the covid-regime States, nor comparing our government to fascists, or bio-fascists. I felt such comparison was as relevant as the Nuremberg Code was to covid shots. Four years later, I was reminded of this censorship with the commencement of the Andrew Bridgen libel trial, as the opening arguments were made in June 2024:
5. Mr Bridgen remained concerned about the risks and side-effects of covid vaccination, and was investigating the evidence about them. At the end of 2022, he raised the matter in Parliament, including by way of an adjournment debate. On the morning of 11th January 2023, he tweeted out a link to an article suggesting a US study indicated links between vaccination and a range of serious adverse health effects. His tweet commented: ‘As one consultant cardiologist said to me this is the biggest crime against humanity since the Holocaust.’
6. At Prime Minister’s Questions later that day, Mr Hancock asked: Does the Prime Minister agree with me that the disgusting, antisemitic, anti-vax conspiracy theories that have been promulgated online this morning are not only deeply offensive, but anti-scientific and have no place in this House or in our wider society?
The Prime Minister replied: Can I join with my Rt Hon Friend in completely condemning those types of comments that we saw this morning in the strongest possible terms. Obviously, it is utterly unacceptable to make linkages and use language like that, …
7. Immediately afterwards, Mr Hancock tweeted out a video clip of that exchange, underneath the text:
The disgusting and dangerous anti-semitic, anti-vax, anti-scientific conspiracy theories spouted by a sitting MP this morning are unacceptable and have absolutely no place in our society.
This is the tweet of which Mr Bridgen complains in these proceedings.
8. Mr Bridgen had the Conservative whip removed as a result of his own tweet of that morning.
The judge found that Hancock’s rhetoric par excellence was not defamatory. The grammatical fact is Hancock, a sitting MP, attributed the property of anti-semitism to Bridgen’s concerns as if it were State-approved fact. It was fact enough to be parenthesised by Bridgen feeling the condemnation of some holocaust memorial and Jewish organisations, and losing the Conservative whip on 11.2.24.
The Holocaust Educational Trust at 1216 hours, 11.1.23 on X. It seems to me, if anyone was co-opting Holocaust symbols irresponsibly, it was Hancock.
It must be understood Hancock did not state Bridgen was anti-semitic, only what Bridgen said was so. Except Bridgen did not say it. He quoted somebody else saying something decidedly not anti-semitic. Bridgen’s quoted consultant cardiologist was in fact not even making a comparison with (nor co-opting) the Holocaust. The Holocaust was a marker in time, indicated by the word, ‘since’.
Bridgen’s act was not even a criticism of semitic-ness, it was a transmission of a doctor’s reasonable, thought-provoking statement about a terrible chapter of discrimination, ill-treatment, human medical experimentation and death in European history. It was not said they were the same or comparable. The reaction of subjective offence from Hancock to Bridgen seems lazy, opportunistic, highly irresponsible and wholly inappropriate. Almost child-like. But, it was too late: a political assassination by a thousand off-point cuts, parliamentary privilege and innuendoes had already been expertly executed.
The Prime Minister may even have been uncommonly and unintentionally correct in saying, “Obviously, it is utterly unacceptable to make linkages and use language like that…”. Was this more true of Hancock or Bridgen? Was Hancock hiding his covid crimes behind a trope of anti-semitism?
What makes this ploy seem worse is the push for jabs, lockdowns and a digital incarceration appeared particularly rabid in the State of Israel, against ordinary Jewish subjects. For those who remain viscerally offended by ‘linkages and use of language like that’, for balance, please read Holocaust survivor, Vera Sharav’s testimony against covid policy.
Hancock’s particularly confusing brand of anti-semitism is borne by confusion from the off. For these days, Jews are anti-semitic, a critic of the political State of Israel may also be curiously anti-semitic. Indeed, Semites are anti-semitic. Despite the confusions, it is clear open dialogue is dead, in part due to the abuse and misappropriation of anti-semitic tropes amongst other -isms. It is as if one is gagged from preventing a present and future atrocity by the political appropriation and hijacking of a prior human atrocity.
What is it about covid, vaccines and semitism which made Hancock’s ruthless, incorrect deployment of these into one trident of spikes bonded by a handle of ‘conspiracy theory’ such an effective weapon to skewer Bridgen upon? Is it a triumvirate of sacred cows whose impeachment is tantamount to blasphemy? Are the popularised anti-definitions too broad or too uncertain to be reasonably engaged with? In life, what stands as truth often seems more visceral and self-interested than it is logical or reasonable.
There are, sadly, many mass human atrocities. Of Zoroastrians, Armenians, Yazidis, Native Americans, Aborigines, The Holocaust, The Holodomor, Stalin’s and Mao’s purges, The Spanish Inquisition. Of Covid vaccines and Covid lockdowns (perhaps at least 17 million and counting, beyond 31 million), of The Palestinians. Genocides for fear of genocide, in self-fulfilment of prophecy. All seem to have political tyrants fronting a mass movement permitting a State to kill subjects. To place one perceived atrocity alongside another in contemplation of the human horror seems reasonable and constructive.
Professor Haim Bresheeth, academic, arrestee of The Met & son of Holocaust survivors provides important counterpoint to Karen Pollock & Hancock. His case was referred to the CPS.
One only has to scratch the surface of Jewish history in the UK to see what the ‘othering’ of a group on the basis of a State-propagated myth can do. Blood libel led to the 12th century pogrom against and (yet another) expulsion of a people from these English shores, that time slurred as child killers. It was a ritualistic mass othering by propaganda and rumour-mongering. In the 14th Century it is said the Jews, having been massacred by Crusaders on their way to fight with the Ottomans, were then accused of spreading the Plague by poisoning wells across Europe. Again, persecution and expulsion followed.
We were all in a sense othered by the elites of the State with the myths of pandemic. The industrial-scaled othering of the millions in the non-jabbed community occurring in the first part of the 2020s happened with the myth that we would kill the State-favoured and Pharma-protected Jabbed. Kill granny and little handicapped Johnny in his wheelchair. The truth maybe that State-Corporate complex is killing us all. There was an utterly irrational, deadly and vicious denial of freedoms, access to general life and healthcare for otherwise well people. Access being contingent on obedience to porous face cloths, fatal covid jabs and fallacious PCR testing.
The matter of Bridgen’s real, reasonable and realised concerns is not reasonably reducible to nation, race, religion, or nonsense, in the malicious, incorrect way Hancock reduced it. Bridgen’s concerns transcended these. What would the medical regulator do to his anonymous consultant cardiologist should it ever find him/her? Their concerns are for collective humanity being forced into a roulette of self-harm, and being denied the individual right to avoid it by the very States and fellow humans it trusts to protect it and its rights to bodily self-determination.
Most-persecuted and anti-semitic person of the year 2024, award-winning journalist Candace Owens. An extreme and unpleasant result of ambiguous anti-semite definitions which may lead to absurdities, and counter-productive outcomes for Jewish causes. @StopAntisemitism may be guilty of #StartingAntisemitism. This humiliation and shutting down by tarring with feathers happened to unlike-minded doctors. DEI should not be a one-sided coin, especially-weighted against traditional believers in DEUS. A reasonable, free discussion of the facts ought to suffice.
Unseasonal novel outbreaks and Changes to Death Certification
In spring 2024, amidst concerted attempts by the State and media to re-ignite Monkeypox scares. There seemed a correlation with Covid boosters and unusual, unseasonal novel outbreaks of whooping cough and scarlatina in adults and children during the month of May, with people randomly pulling out laid-off PCR Covid tests and testing positive for that, too. The obvious question not being addressed is, are covid boosters making the world iller? The insanity continues unabated elsewhere:
April 2024, an 80 year old is hospitalised by septic shock due to acute diarrhoea – diagnosed as campylobacter enteritis, but, because there is a surge of coughs her septic screen includes covid testing. She ends up also on paxlovid in spring 2024 – obliged by a clinically meaningless test done inopportunely and inappropriately. This is a veritable medical mess and morass of confusion.
In June 2024, another man, 82, may have had a mild CVA, he is admitted and diagnosed with a CVA. Incidentally, he tests positive for covid on the stroke ward. He is asymptomatic for respiratory tract infection, but that does not stop the doctors administering a dangerous statim shot-in-the-dark of Sotrovimab, trademarked, speculative, intravenous monoclonal antibodies. In a letter sent separately from the hospital discharge note, the hospital administrator explained, ‘Sotrovimab was given as per hospital policy’. Individual clinical care should not be corporate policy-driven. These are not the normal behaviours of physicians nor hospitals.
There is another twist, the patient’s daughter is a colleague. She is completely unaware the presumed antiviral biologic, Sotrovimab, was inappropriately administered. She is shaken, and remarks her parent has not been the same since that admission for a mild, non-infective, embolic CVA.
Later that year, the law that issuance of death certificates (MCCD) was only to be done by the last attending physician is changed. Now, ‘Any medical practitioner who has attended the deceased within their lifetime can complete an MCCD if they can establish the cause of death to the best of their knowledge and belief, and the death is not required to be notified to the coroner.’ There is a medical revolution afoot. Not knowing the patient during or proximate to the last illness leading to death inevitably blurs true knowledge, and the ethical imperative for precision in deciding the cause of death.
Another colleague knows of three recent, new diagnosesof profoundly rapid and disabling motor neurone disease, post-jab, locally. That is an abnormal rate. These are not likely by chance. Four years later, the suppressed immunological explanations follow the suppressed facts and the jabs. It is a warp-speed recipe for inflammation and immuno-tolerance with the potential results of ‘turbo-cancer’ and systemic autoimmune disease seeming to be realised.
“The Pfizer jabs are all full of SV40. SV40 was what we put into mice to make them grow tumors…and we’re putting this into humans… These people behind Moderna and Pfizer are just pure, pure evil…and they must be held to account…” Professor Angus Dalgleish, Oncologist
Picture all those elderly people in residential and nursing homes, swaddled in blankets on well-worn recliners and medical-grade mattresses. Too trusting, weak or out of touch to resist. Still wallowing in the reverberations of baby-boom hope from a post war Europe. They are the internet-deprived millions still accepting the covid jabs like one of those semi-transparent plastic beakers of lukewarm tea held tenderly at their supping lips.
The government will know of all this democidal iatrogenicity. A few clicks on NHS Big Data, to track contemporaneous blood counts, anticoagulant prescriptions, morbidity and mortality and other parameters, then overlay the rate of covid jabs, and covid policy and one will see the effect of the global attack by our Frankenstein States.
It was all so obvious to a mediocre doctor such as myself. Whilst I predicted and observed a slow car crash of medical incompetence and denial, most of my colleagues did not seem to acknowledge the madness, nor notice the patterns of covid jab complications. However, they cannot feign ignorance of basic medical ethics and safety. Those not accepting this alternative universe has any validity, please note the evidence continues to mount behind invisible information barricades. Take this, for instance, from the North Group, or this important scientific paper:
It is not public policy for governments and medical regulators to accept reality. “We call for an immediate halt of all RNA-based biologicals until these concerns are scientifically addressed and convincingly dispelled.”Link to full paper. If they are so safe why has Biden’s parting shot been to extend the liability shield to Covid jab manufacturers until 2029?
Covid ideology weaponises collectivism. It will be weaponised further to remove everyone’s human bodily sovereignty and autonomy. The spike-injected will not be spared in the longer-term. Individual rights such as to work, to resources, food-independence, and bodily sovereignty have been eroded by covid dogma. So have national sovereignties. It is a supranational communism for the masses refined by elite fascist corporates.
It is a diverse, equal and inclusive attack on all groups. Not only Jews or errant doctors. It is an attack on traditional faiths, belief in fate, belief in self-determination. It promulgates a homogenisation of man, not diversity. It is communism via the back door of fascism. The covid saga delineates a definite food chain. All resources in the hands of a few elite, non-empathic entities. 99.9% forced to feed from a 0.1% digital hand. Forced to call comply with genetic self-harm in order to subsist. A wall of digital bio-compliance is being erected between humans and their natural means to survive.
Our States move increasingly to subdue the masses by legislated censorship, wordplay and brainwashing subjects to narrow the space and spectrum of permissible speech and thought. It cripples meaningful human interaction. It is not the stuff of liberty or democracy. Can mankind fight such overwhelming tides when a portion of the overwhelming tide is mankind? We must not permit basic human decency and our freedoms to be taken away through fear, under a cultural anaesthesia of State propaganda and identity division.
30th December 2024, Dr Dave Rasnick and Michael Palmer, MD, gave their respective views on SARS-CoV-2 and its role in the “pandemic.” Dr Rasnick :
1. There is no evidence of a pandemic (i.e. COVID-19) in the USA in 2020. All-cause mortality in the USA was lower in 2020 than the previous 5 years.
2. There is no evidence that a virus known as SARS-CoV-2 was actually isolated from even 1 person with symptoms, nor even looked for in healthy controls. This is in spite of over 16-million unique sequences of SARS-CoV-2 reported to GISAID as of July 25, 2024.
Michael Palmer agrees with Dr Rasnick’s first point, but not with the second. He provided the proof of the existence of SARS-COV-2 and its association with disease, starting at 13:30.
Final word: Dr Mike Yeadon, Former Chief Scientist and VP of Pfizer’s Allergy & Respiratory Unit. Video: source
31st December 2024
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org.
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, asprescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. These articles are artistic expression, should not be taken on trust, and certainly do not purport to necessarily represent the views of the medical profession nor the NHS. They are not at all intended to replace government health advice. Any patient details have been anonymised.
Part 2, Fifty Shades of Covid Tyranny: The Present
“During the last generations the medical monopoly over health care has expanded without checks and has encroached on our liberty with regard to our own bodies. Society has transferred to physicians the exclusive right to determine what constitutes sickness, who is or might become sick, and what shall be done to such people. Deviance is now “legitimate” only when it merits and ultimately justifies medical interpretation and intervention. The social commitment to provide all citizens with almost unlimited outputs from the medical system threatens to destroy the environmental and cultural conditions needed by people to live a life of constant autonomous healing.
…
Limits to medicine must be something other than professional self-limitation.
…
Professional power is the result of a political delegation of autonomous authority to the health occupations which was enacted during our century by other sectors of the university-trained bourgeoisie: it cannot now be revoked by those who conceded it; it can only be delegitimized by popular agreement about the malignancy of this power.”
From author’s Foreword (1995 edition), Limits to Medicine, 1976, by Ivan Illich
Illich was right, and his wish is granted. Medicine has been removed, with the accelerant of State covid policy from ancient, professional normative values. Illich would, nonetheless, be more unhappy: medicine and the definition of health is now under the centralised, global control and delimitation of a State-corporate-military complex.
Previously, I had written on the strange death of medicine. It is, I realise, strange because it is a transformative event. Some colleagues say it is the ‘America privatisation’ model nearly fully-implanted. It is more than that. It is the reformation of a church. The new, State-nominated priest is the Noctor. I am surrounded by so many, I no longer remember what all their acronyms mean. Nurse ACP & ANP, non-nurse PA & HCA, Paramedic FCP & AP, etc. They seem to know not that much medicine, they have less or no experience of my role, but they do most of what I do, and they are paid less than a GP (usually, but not necessarily). Often, their pay exceeds a junior hospital doctor’s. I believe it is a recipe for poorer individual healthcare provision and iller health.
Even after the independence of physician and surgeon education was adulterated by a Rockefeller petrochemical industry, at least the discipline of meaningful, strict medical diagnoses survived. Post-covid that, too, is gone. Today, it is normal for a worried, well patient to book an appointment simply to tell you they have been diagnosed with covid by a piece of cheap, profitable plastic. The question is begged, What am I still doing here? Catalysed by covid policy,extinction has crept upon UK family physicians like a silent assassin. They were too busy, and self-assured to notice. Other leading and managing colleagues sold the rest out in favour of self-interest, and cheap labour for short term fixes.
The Prehistoric Doctor
At the inception of the NHS, up until the early 1950s, GPs were performing complex emergency abdominal surgeries, and providing the general anaesthesia. GP colleagues working in off-shore Scotland were performing appendicectomies in the 1980s. In the 1990s ‘Clinical governance’, ‘restructuring’ and Calman’s 1995 ‘Calmanisation’ restricted medics’ professional flexibility and self-determination in favour of standardised, accelerated senior career paths to consultant posts. As a junior doctor I had the liberty of doing any job in any specialty at anytime I chose, thus becoming a well-rounded doctor moulded in my own image with the blessing of my seniors. One entered a didactic medical hierarchy … a ‘firm,’ where one lived and died by the professional standards and prejudices of one’s boss, he who ultimately carried a major clinical responsibility for your actions on his patient. It was simple and effective, but not infallible. It did serve to prioritise clinical care over box-ticking.
By 2000, Harold Shipman became the standard by which the UK profession was judged and mistrusted. Naturally, aspiring school students became a self-selected cadre of uncaring, murderous sociopaths; unfiltered and promulgated by medical school selection processes and education. We do-gooding killers had to be stopped by GMC over-regulation and over-reach. Yearly revalidation introduced to placate the public’s fear did nothing to prevent a future Shipman. It simply created a culture of obedience and silence where neither is a professional asset. In that process, the GMC itself underwent a communist reformation to its constitution. Professional values were admixed with lay-person values both in its structure and in the panel of its disciplinary process. No longer would fundamental human rights and the professional ethical judgement of a reasonable body of one’s senior peers be enough. Confected political correctness became king. By 2006 ‘Modernising Medical Careers’ policy had constrained junior doctors to an early choice of specialisation. This was not a good thing: the earlier one is professionally compartmentalised and elevated, the less clinical experience, and the more easy one is controllable.
By 2020 the State of Covid destroyed professional standards of medical safety and ethics in favour of pushing unnecessary, lethal, improperly-vetted injections for profit. It advised normally-competent, caring doctors to suspend standard, simple treatments and referrals for standard symptoms and signs. Most complied, awaiting the miracle gene juice, silently implementing orders, and inappropriately denying care. The irony of Shipman should not be lost. State and doctor, fused, were hurting, maiming and killing.
Now, the premature elevation to professional medical competency occurs before the cradle: non-medical staff are delivering the bulk of general practice patient care. Increasingly, they are not even qualified nurses. This increases the power the State has upon the profession and upon population healthcare. The interests of service providers increasingly trump individual patient choice and the wisdom of professional medical experience and seniority when it comes to each patient. One of the most remarkable inverse trends this millennium has been how wise senior professional colleagues are seen as old nags to be worked to the bone on basic service provision until, the final journey to the glue factory. Old, wise doctors are expected to work and be treated like young, inexperienced ones. It is humiliating, inappropriate, and injurious to the profession and to patient care. Both are now in decline and crisis.
Over my career, dedicated consultants’ offices, their secretariats and car parking spaces diminished, while managers installed and expanded theirs. It always struck me as contrary: surely a hospital without doctors at the vanguard of patient care is a non-starter? A de facto Manager-Patient relationship was born. This was sold as beneficial to the profession, but it was more beneficial to hospital administrators and politicians. After a life in the profession our seniors’ experience and confidence is subversive to management, and so that natural authority is now managed into the ground. In the NHS, Field Marshall Montgomerys are being sent to muck out the barracks’ latrines, day in day out.
The changes of the last four decades have dumbed down the profession, reduced our autonomy, and handed the mantle of our ethics from the ancient Greeks to Pharma and politicians.
A Country Practice
A senior GP colleague, living in his community, and being doctor to most of it for over 30 years, including to said patient. His neurologically-compromised neighbour falls, and lacerates a shin outside the front-door. It is wintery. An ambulance is called. An off-duty hospital nurse arrives, then a ‘fast-responder’ in a fast-looking car, and then, a blue-light ambulance. The off-duty nurse says the haematoma requires hospital. The fast responder says there is no way ‘Health & Safety’ would permit him to lift the man off the stone-cold pavement. He calls for a precious paramedic crew and their blue-lit ambulance to whisk him an hour to the nearest hospital. The fallen man does not wish to go, but goes by tick-box exhorts above common-sense. Amidst a sea of centrally-controlled, State algorithm health implementers, there has been standing an older man in a dressing gown, drinking his Sunday morning mug of tea, He is the off-duty GP, and neighbour. He says it did not require hospital, or an emergency. Someone in authority simply had to agree to take him back inside to the warmth of his house. No one listens to the man once-heard. He is, these days, a State-neutralised, decentralised, autonomously-thinking threat. No longer relevant, no longer audible. Another extremely respected GP colleague and mentor has fled after 35 years service to become a fast responder. A first aider with a car and oxygen. Imagine her patients’ faces. She will be compelled to train for the noctor privilege with a six month starter course. Individual agency in the West is at a nadir. We have reached a point of collective cultural insanity and conjoined infantilism.
The current state of the State NHS: a paradigm shift in doctoring
Covid policy has hastened a paradigm shift in healthcare. But for the majority who are rendered reliant upon State medical services being fearful, elderly, impoverished or cognitively impaired, the State could not get away with it all so easily. Medical colleagues do not help. Many continue to be blinded by, base themselves within, and celebrate being part of a politicised medical system counterproductive to health but conducive to status and profit. An unrealistic system of healthcare and healthcare regulation which regularly abuses and humiliates both those delivering and those receiving healthcare. It is a system which has recently been extremely damaging to society.
It is not only the medical paradigm. Everything has become the worst version of politics. Science is conducted politically, as is teaching, policing, justice, and journalism. No one in any position of professional authority within these professions which are based upon ethics, honesty, logic, openness, critical thinking, and due process is employing those techniques properly. Rhetoric, sophistry, and emotional manipulation are all they need to keep rising to the top. Any doctor or nurse who points this out is whacked by the system and by colleagues. The noble and courageous Dr David Cartland is an exemplar of many cases in point. It would not make sense in a normal world to silence, threaten and destroy a canary in a coal mine. It is a subversion of a natural order happening in all disciplines everywhere in the West. A symptom of a crashing financial system, led by the greedy with no idea except of tyranny. They cannot hear that they are wrong, and should be gone.
Whether one believes covid or not, amidst dysfunctional, crashing NHS computer systems which operate slower than the stressed NHS employee can think; and serial junior doctor strikes for non-living wages, it remains true that healthcare has been industrialised, centralised and moved away from the realm of qualified doctors, beyond the pale of ethics, rights and morality. A political-corporate tail wags the medical dog.
At inception there was no NHS pushing of anything, only a pushing of patients away. Even patients apologised for attending and using a precious, new social resource. Now everything is pushed to ensnare patients for third party benefit. There has been an expansion in group SMS contact with patients for agendas not driven by the patient: come measure your cholesterol, come have your jab, come have psychological reprogramming for jab hesitancy, be part of our research study, or please don’t bother us today for we are too stressed. There is reducing State interest and incentive for patient-initiated contact. Instead, why not visit the self help app, or endure the auto-consultation followed by, if one is lucky enough to get through, a telephone-whipping from an automaton.
Take, for example, an invitation to our practice NHS ‘well-person nurse examination’. Behind it is only one outcome for the doctor. The invitation consists of only one strategic blood test: a cholesterol screen. Then, an inevitable, potentially anxiety and statin-inducing, QRISK calculation by the healthcare auxiliary, followed by a mandatory appointment to the doctor. The doctor has a difficult conversation with a patient if she dares be honest about the facts. She is under pressure to prescribe. Everything NHS is tending toward State-corporate agenda-driven medical contact.
Seniority: a distinguished NHS doctor politically extinguished
One of my more learned NHS colleagues, now former NHS colleague, was snuffed out a year ago. He is a surgeon, hard-working, dedicated and caring. He kept a department alive for two years whilst colleagues ran away because of their ethnic covid risk, their blood pressure, or their ACE inhibitor prescription being catastrophically linked to a said spike protein affinity for ACE2 receptors. We might forget how bad the madness was. Some of these colleagues continued to feel safe earning in private practice.
During this covid saga, my colleague noted a dangerous clinical-prescribing error, also conflicting with departmental guidelines, by a consultant colleague 15 years his professional junior. My colleague sent a generic, non-confrontational email asking colleagues to take note of the guidelines. No inquest or meal was made of the specific error, no particular colleague made to feel humiliated. One year later he was hounded out of the NHS, and is now close to retiring outright 15 years before his time. He has no interest in private practice for profit, only in helping those most in need.
The junior colleague (a newly appointed consultant) who had made the error, complained that the senior colleague had used the term ‘Junior Consultant’. Another (senior) consultant colleague conducted a year long inquisition, and asked the other consultants to provide other evidence throughout my colleague’s 15 year tenure of other such documented examples of subjectively-offensive, correct use of English. There weren’t any. The reasoning applied in my senior colleague’s case decided, ‘We are all consultants, there are no seniors or juniors’. Are we not all also doctors? Triggered junior (sorry) doctors may have found another reason to strike.
My colleague was compelled to apologise to the junior consultant for his correct, inoffensive use of the English language in an English NHS hospital. He did, and then immediately resigned. This exemplifies a now commonplace, self-policed tyranny. On this occasion it was the linguistic communist strain of it operating in the modern workplace. Even more incomprehensibly, his shocked clinical colleagues and clinical manager asked him to reconsider this reasonable, objective resignation response to an unreasonably held, subjective offence. The result is another un-doctored, senior doctor. Society is eating itself, and the State aids and abets it.
A Medical Extinction event
I have noted a degree of online disquiet in GP social messaging groups. Non-doctors are increasingly practising as if, and in place of GPs. Someone on a group refers to them as ´Noctors´. Non-doctor doctors. GPs are now performing only 40% of the GP consultations in UK practice. Pre-covid, back in November 2019 it was 50-52%. This is not all. Factor in a greater proportion of this 40% being, now, conducted remotely by GPs. GPs who may be contracted through remote, third party organisations. Sometimes, they are working from abroad, and have no prior working knowledge of the community, culture or individuals, and still work to ten minutes-a-patient. This is far from the ideal of the UK GP doctor-patient model. In this, a highly trained and experienced GP would know each and every patient, many from birth. The GP would see patients in vivo – the least risky, most efficient and most rewarding way for all concerned. The brief contact was compensated by more available, frequent contact. This reduced anxiety, and increased accuracy of diagnosis and safety of treatment. The results of this change to doctoring, witnessed first-hand, are distressing, dangerous and shocking.
An isolated old man languishing on a worn-out couch, not seen for months, telephoned only by a remote, third party colleague unknown to any of us. A casual treatment of undiagnosed, severe leg pains by morphine; doubled the next week by the same telephonic negligence. The immobilised, elderly patient hallucinates and calls distressed. It is clear the patient is at risk of several underlying pathologies which may have required an emergency ambulance weeks ago, and for which morphine is entirely inappropriate and hazardous. All this would have been obvious with a casual, caring glance at the complex notes or by a familiar GP, or if the doctor were present. But this GP is remote, cold and on autopilot, churning rapidly through the numbers to appease the system at the expense of a patient.
It does get worse. Imagine now only replacing the doctor with a noctor:
An elderly patient, unseen for a year, except by a series of noctors who take bloods and procrastinate, ‘repeat urea & electrolytes in two months’. The noctors are reassured, ‘U&Es stable; repeat in two more months’. This carries on for a year. The problem is the patient’s renal function suddenly plummeted one year ago from normal to 90% less, and to the brink of dialysis. No one understands somebody needs to do something else. I speak to the elderly wife of the patient, chance-referred to me by a concerned community worker. She says, ‘Doctor he hasn’t been seen by a doctor. Nurses just keep taking bloods.’ I do not blame my colleagues. We are in increasing crisis, I haven’t had a lunch break for four years, and often struggle to find time to visit the toilet. Like a workhorse with a nosebag, I can eat and drink as I work, but I draw a dignified line at catheter and leg bag.
Most of my patients do not even notice the noctors are not doctors, nor do they seem to care. Some noctors are more bogus, and introduce themselves as ‘part of the medical team’ or ‘Generalist Practitioners,’ even if neither doctor nor nurse. Everyone seems to be in the process of being permitted some kind of prescribing liberty and professional loosening-of-association. I know too much, and I know what I do not know. I would think thrice about prescribing on the phone without physically seeing patients. A picture paints a thousand words. Noctors with little knowledge or experience seem incredibly comfortable with prescribing like this.
This should be unsurprising, since covid. I witnessed in one UK NHS general practice the extraordinary spectacle of our janitor and social worker being pressured by management into injecting the immuno-compromising, genetic elixir of spike protein into my patients. The social worker was un-jabbed, and the janitor broke into a sweat and demonstrated a greater sense of medical ethic than my collective profession. He said, ‘No way. That’s not right’. Correct.
I say to my colleagues and the Royal College of General Practitioners, it is our just dessert. Our complicity in political lies, assistance in the destruction of our medical ethics and the sacred relationship of trust and confidence with our patients is unforgivable. Most of us have become de facto Noctors. Deserving of the title for behaving in a most un-doctorly way during covid. Transforming into unethical, weaponised, uncritical and obedient State instruments, precisely when one should not have, qualifies one. Many basked in the glory of being a frontline hero in a faux crisis. If an entire profession and its leaders say nothing, and behaves as if corporate technicians, it deserves nothing. The system has found a more desperate, cheaper, less-regulated and equally unethical technician to replace you. Soon, AI will replace all that. We will all go the way of shorthand writers.
Who are the Noctors? What is ARRS?
In my locality, not only are we losing auxiliary and clerical staff to the local weapons industry which is busy ramping up munitions production for WW3, but paramedics now do the bulk of routine, non-urgent GP home visits for chronic disease. They have replaced the dwindling availability of GPs. At a time when the job is so stressful and unsatisfying, many are leaving or working less to protect their health. Once upon a time, paramedics were the experts in pre-hospital emergence care, and we were told in the severest tones they should never be bothered or have their time wasted by chronic disease (‘see your GP, you time-waster’). They were said to be too busy rushing in-between emergencies and Emergency Departments.
Nurses now perform much of the general practitioner work, particularly the routine chronic disease management of diabetic and respiratory disease in clinics. We no longer have enough nurses to deliver this care, and GPs complain it is not what they do, anymore, as they have become deskilled. This is true. But it can easily, and may have to change. In addition to paramedic and nurse noctors we also have the launch of NHS Pharmacy First advanced service, which inverts the classical ‘history-examination-diagnosis-treatment’ model of medicine on its head: this year the frustrated patient and embattled GP receptionist will have to decide on the correct diagnosis for it to correctly arrive at the threshold of the inexpert pharmacist. GPs have already raised concerns about this scheme.
GMC regulated Physician Associates
A more controversial phenomenon is the rise of the non-medical, non-nurse and briefly medically-educatedPhysician Associate to add to the NHS armamentarium. Already, there have been PA disasters, and there is increasing confusion and concern. PAs are being promoted by the government funding policy, ‘The Additional Roles Reimbursement Scheme’ (ARRS). This has made available to GP surgeries £1,412 million in 2023/24 to employ people in 17 new roles. GP surgeries were excluded from using this money to pay for practice nurses and GPs. Some practices that are short of funds are relying on ARRS funded roles. GPs are panicking, petitioning and crying ‘employment crisis’ too late. But, deep down, one should know from covid that resistance is futile. The blurring of professional boundaries is becoming extraordinary. PAs soon may become GMC regulated. In reaction, doctors’ bodies threaten the government with legal action. I suspect GMC-regulation is a way of giving PA’s prescribing rights, since all PAs need to find a way to prescribe is a HCPC regulator. It is also another self-fulfilling prophecy for GMC self-preservation.
The dangerous defunding and un-doctoring of general practice is recognised as serious by the BMA, which released this strong message about the upcoming unacceptable ‘new GP deal’ being tendered by the government. The matter is going to a GP referendum on the 1st March 2024, in an election year. GPs seem serious about a remedial response if the government will not heed their sincere safety warnings.
One might see where this is going. Soon, GPs may be doing less than 25% of GP consultations. The General Practitioner role is becoming extremely generally practised by all-comers. In one English general practice, 11 GPs were ‘offered voluntary redundancy’ in favour of ARRS staff roles created through ‘new (unsustainable and unsafe) ways of working’, three GPs walked. Since covid policy it has become a free-for-all. How soon is it before the pharmacist, paramedic and nurse are also refusing to see patients to the face, or complaining they are deskilled in their traditional purpose? How soon before all these, and the physiotherapist all decide leaving their professions and re-qualifying as a PA is the way forward?
It is not an efficient nor resilient model. A paramedic attending a complex, chronic disease or palliative care case, traditionally the remit of a non-urgent home visit by a GP is not appropriate. Paramedics in a case like this can often only safely do nothing but report findings. They, via messages passed to over-worked GP receptionists, who in turn suggest an over-worked GP, given none or a maximum 10 minutes’ grace, should remotely respond or prescribe based on a vicarious, inexpert examination and opinion. It is as if a phantom visited leaving a phantom diagnosis and a phantom treatment. The only safe alternative is a morale-sapping reduplication of all the work by an increasingly side-lined, demoralised GP. A car mechanic or vet would deem it unsafe to work like this on your car or your dog.Why should humans deserve less?
The noctors or their unsuspecting patients often and eventually have to defer to a doctor. Often that point is when the patient is feeling far worse. Fortunately, there remain a few older GPs with sufficient experience to shore up the chaos and conceal it from manifestation. But they are dinosaurs entering an ice-age in a medical extinction event. They are fleeing, retiring and reducing their hours just as they are being replaced with technicians paid to follow algorithms. I, a Hippocratean anachronism, have chosen to work increasingly, and voluntarily in the more wise and respectful ‘less-developed world’. The doctor-patient relationship, and application of basic knowledge and critical thinking stills applies there, but it is so yesteryear, here in the UK.
There has been a planned intent to de-doctor the NHS for many years. Consider ‘A Roadmap to Practice’ for the plan of Paramedic First Contact Practitioners (FCP) and Advanced Practitioners (AP) in Primary Care, or the NHS Pharmacy First advanced service. View these within the government proposals to regulate all healthcare professions under one monolithic regulatory body and one code, and you will realise the Hippocratic doctor is nearly as dead as a dodo.
Where is our profession’s future, when there is no future? I suspect if newer-trained doctors are as dumbed down and ethically unconscious as the society they are reared in, so the gap between them and noctors may not be as great as with old schoolers. Junior doctors may still believe in their doctorly omnipotence. They strike for their rights, and clamour for rewards for compliance with a medical tyranny they do not even know has occurred. Many seem to leave the country, the profession or avoid general practice entirely. They do not seem to realise recent history and present trends. Their entire didactic tradition of medicine is being demolished and replaced with low-paid technicians, who are even more likely to obey, and perhaps less able and less likely to criticise government medical policy.
Noctorism
Noctorism is destructive to professional boundaries, ethics, efficiency and expertise. It furthers the destruction of the culture of a professional hierarchy of learning and quality control. Imagine an army with an inverted, a muddled chain of command, faulty systems and no funding. I hear regularly of a variety of noctors, undermining doctors’ decisions based on flowcharts, or miseducation rather than clinical nuance. They return patients for another unnecessary consultation. It can only end in a continued NHS chaos that hungry corporations will inevitably be commissioned to replace and parasitise upon. It is not merely a NHS tending to the private American model. It is more profound. It is the marginalisation and eventual death of the physician. Surgeons will survive, for a little longer. The next step will be the permanent end to the physician-patient medical model. Enter a pure corporate, Big Pharma-patient model: a non-Hippocratean, non-medical technocratic medicine delivered by AI automatons.
This is a brave new world where ambulance crew are GPs, State GPs are killing you softly, men identify as female babies, teachers and the Tavistock transmute little boys into women whilst your geo-tagged courier flings your parcels onto the ground and flees. Nothing does what it says on the tin anymore. A world where the democratically elected politician determines the Truth, and decides what you can and cannot think. It is a topsy-turvy world where there is no right to voice a professional opinion subjectively offensive to the state.
After three decades, I regularly feel unqualified and incompetent to be part of the medical profession. A veritable medical imposter. It is the price of circumspection learned from being an expert in managing medical uncertainty and life-death decisions at their riskiest, in the community. My observations tell me so should many more of our inexperienced noctors, although many appear to not. The new noctors appear less stressed than me and seem to deal with serious clinical conditions with less concern and effort. It may be understandable, they do not carry the can, nor will they know what they don’t know they are missing in their management. Or are they simply better than me? Meanwhile, we are expected to supervise, and take responsibility for their mistakes, while they are the seed sown for our demise.
The responsibility and stress of general practice is overwhelming, particularly in a collapsing system. Unfortunately, the rise of the noctor inevitably makes the general expectation of standards within and upon the GP profession lower. Less of one’s colleagues notice or care about one doing the wrong thing. To put it another way, would one be happy for a GP to be repurposed into a non-scientist senior scientist, a non-paramedic paramedic at a pre-hospital multiple trauma, the non-dentist dentist drilling your teeth, or to be the non-nurse nurse nursing you?
Many GPs and hospital consultants seem happy to be siloed behind phones, attempting to ‘see’ patients ‘telephonically’. None of this was conscionable pre-covid. If the profession continues to support this unprofessional attitude, it will find it is deservedly losing its professional territory, and those patients to private and enterprising hassle-free paramedics, GMC-regulated PAs and nurses. It is a shame-worthy situation for the GP profession. We should be unsurprised if we are sent to drive ambulances to emergencies, replace striking juniors in emergency departments, and performing nursing and phlebotomy services. GPs have been time-stressed so much over recent years they have been gladly ceding work to a Trojan horse, but soon we may have none left. Old GPs may be soon all be working from and seeing their ex-patients in A&E departments, deputising for migrated and striking juniors, and perhaps mopping up after a deserted, noctor-led general practice system in private, doctor-led general practice.
State-engineered System Chaos
If one is not allowed to deliver individualised, nuanced and intelligent medicine the result is as we have already witnessed in covid: a centralised and widespread algorithm of State policy-worsened health. The noctor-technician policy will only worsen the problem of a reduced long term patient knowledge of and continuity of holistic care for a patient which used to be the hallmarks of the old family doctor-patient centred model. This will lead to more unnecessary investigations, less working knowledge of each patient and consequently poorer, less focused care with more consultations. It will cause more error and more over-prescribing. There is already a distinct feeling patients are increasingly being looked at as beans to be counted, then stewed, as inappropriate, in an official formulary of chemicals.
Those who think that noctors are not being pitched against GP or hospital doctors, be made aware their provision is in this way also undermining the training of junior hospital doctors. Often noctors are too busy being doctors to perform their core clinical activity. For instance, one consultant colleague reported hospital opticians are too busy being and supervising junior ophthalmic doctors to provide refractions for her. Even teachers have become noctors, and their schools health modification facilities during covid. They undermine parental and child informed consent, and doctor-patient-parent relationships in favour of State-pharmaceutical agendas. Complementing allied professionals is one matter but up-ending our profession and our training structure with noctors is an existential attack.
It does seem doctors have become too over-qualified for their own profession; but why have a qualified, responsible and accountable named-physician when one can instead have multiple incoherent, over-investigating, under-qualified individuals working without direct accountability within in a State-created crisis?
Unintelligent, State-confected over-investigation is causing chaos, rather like the recent covid PCR False Positive Pseudo-Epidemic as explained here by Dr Mike Yeadon. Ultimately, any such attempts at decentralising and decerebrating a clinical diagnosis only benefits those corporations and State actors that politically and financially prosper from the pharmaceutical and pandemic business.
The problem is global. The WHO and Public Health are also anti-doctor and pro-noctor. WHO director-general, Tedros is a noctor, as are many who have quietly displaced doctors in leading community public health posts in the UK and worldwide. Any lukewarm, non-medical, compliant body in a medical position seems to suffice for the hygiene socialists. Thus, ailments are less and less being seen as personal healer-patient issues with optional, ethical individual solutions. They are, on the contrary, being seen as public health issues with technocratic, veterinary group solutions.
Farewell, Doctors
This new, noctor revolution is reminiscent of the back-protecting NHS Direct (and its successor, NHS 111) which, in 1998, instead of reducing GP and A&E attendances increased them, societal medical neuroses and individual dependency upon the State. ‘Lay referral system’ is no-longer a thing because of it; and because the family and community units have been State-shafted. Less State intervention was far more more effective than NHS Direct. The same will be said of the supplanting of Hippocratean doctors, by lesser, State-obeisant colleagues, and now, with noctors. I fear it will make an already noxious State healthcare provision dumber, less-efficient and more dangerous.
There are excellent noctors, but they are the exception, not the rule. They should not be presented as a replacement. In a sense they should have been doctors, and some do re-train. It is not a wisdom that brickies or road-layers should be given a fast pass to civil engineer. Why is it wise for medicine? I do not believe good safe medicine can occur like this. I know senior nurse colleagues who agree. I suspect it is desperate and wilful State crack-papering and can-kicking. Surely, not even noctors would wish their system of healthcare upon their families?
I do not advocate for doctors and allopathic medicine at all costs. There are far better alternative approaches for many conditions. Whatever one thinks of the GP model, it is efficient in doing most of the NHS’s work for a tiny proportion of the NHS budget. Change that and one is left with a dumbed down, problem-creating machine. Consider where a GP is purported to deal with a complex case in 10 minutes with all the administrative and preparative work included. Here, a lawyer would justifiably charge three hours work for those three phases of work to do it carefully and properly; and, if a patient tries to lever five problems into that rare appointment, a lawyer would relax and charge five times more, and prepare for a rich season of regular, escalating work.
I know some PAs are being offered £80k per annum for a 40 hour week on the locum market. This is a GP salary, without the skill, responsibility or stress, and no need for a loan for nursing or medical school. Such incentives are destroying the core of the traditional and well-tested medical model and replacing it with an unsustainable, unsafe bureaucrat’s pipe-dream. It is so nonsensical, one must ask, is this move to counter-productivity deliberate?
The hallmark of a doctor should be an intelligent, caring, critically-thinking, autonomous, ethical, safe decision maker. One of the most effective medical and social acts of a general practitioner imbued with the status of professional medical learning, experience and ethics is impactful patient advocacy. This is no longer allowed to be the case. One needs only consider the wicked government covid jab non-exemption exemption scheme. Where was the profession for those intelligent patients who knew something was not right with the jabs? If the vocation is a medical free-for-all with no firm ethical code, no one respects or trusts anyone.
The profession and our regulator deserve to now be recast into something better. Putting one’s professional house in order requires introspection. When one points the finger, few retain the insight to realise three fingers point to oneself. Medicine’s decline is medicine’s fault.
I cannot care about a medical profession and regulator which does not care about its own core ethics. Our noctor nemesis has not even a cultural memory of ethics. The profession must decide, and do or die. The monopoly is already broken and was never, in itself, important. What is important is medical ethics, at the root of which rests an essential humanity and intuitive morality. This is our profession’s ancient, decentralised moral cryptocurrency which the State is desperate to destroy.
Beware, other professions, you are not immune and the medical revolution does not stop: Dinosaurs! Make way for the ‘Medical Apprentice’!
“General Practitioners dominate primary care by right of an inherited tradition, because they are there. This situation won’t last; if doctors are to retain a leading role in the future, they’ll have to earn it, and if some other kind of health worker can do better in terms of measured health outcomes, good luck to them.”
From Foreword, ‘A New Kind of Doctor’, 1988 by Dr. Julian Tudor Hart, FRCGP, FRCP
28th February 2024
Life mirrors parody. Any (equally fake) registered doctor and noctor who supported, complied with, remained silent about and advised lockdowns, masks, treatment coercion, denial of choice, standard treatments and fake experimental, unnecessary covid pseudo-vaccines without adequate testing and proper informed consent need not attend. MHRA, EudraVigilance and VAERS figures, Astra-Zeneca vaccine’s procrastinated UK market withdrawal and UK excess mortality figures cannot all lie, no matter how hard the ONS tries to reimagine the data.Concern continues to be expressed as to how junior doctors will learn, subsist or co-exist with the noctor.The GMC and Noctors are both State weapons against doctors and population health. PAs may not yet realise the GMC may also become also their worst best friend. They will have to pay (hopefully the same as doctors) for the privilege of the instant karma.Some doctors are grumpy but remain largely politically naïve.Non-doctor doctors. GPs are now performing only 40% of the GP consultations in UK practice. Pre-covid, back in November 2019 it was 50-52%.
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org.
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, as prescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. This article is an artistic expression and personal view of life, should not be taken on trust, and certainly does not purport to necessarily represent the views of the medical profession or the NHS. Any patient details have been anonymised.
Part 1, Fifty Shades of Covid Tyranny: The recent past
The Scream, by Edvard Munch
Still here at the ‘frontline’ of nothing. Still un-jabbed, unmasked, and more likely to be killed by jabs, State covid policy and State persecution than a putative coronavirus. Still alive. Still thriving. Physically, and spiritually, if not entirely psychologically. Still fearless of everything but people’s blind obedience to a State policy of catastrophising.
Reality-Enforcement through Policy Trauma
Hypervigilance, avoidance, flashbacks, nightmares, anxiety, depression, loss, denial, anger, guilt, grief. Just as being physically unwell should not be thought the norm, so these are not normal, chronic states of mind. Yet this societal psychological (and physical) dysfunction is being normalised by our States. The prevalence of these symptoms of psychological trauma sky-rocketed during the tyranny of covid. A significant proportion of a generation of children no longer attend school due to severe neuroses generated by covid policy.
COVID-19 is far more bureaucratic policy than disease. Covid damage is due to policy. The covid grim-reaper’s respect of national bureaucratic, statistical and political borders indicates this. The consequent trauma runs deeper than a World War, but in covid there is no closure, no reasonable explanation, no identifiable enemy, no day of reckoning. Merely an unjustifiable and traumatic move, in concert, by States, to fundamentally change the meaning and function of all things.
In late 2019, plans for the world’s largest cosplay event were finalised, rehearsed, and then activated through a lock-stepped global, undemocratic policy cascade determined by corporate and private bodies using the same phrases and ploys. It was an awesome, mafia-style implementation of their convenient truth. We were psychologically reframed and transformed by orchestrated, internationally-ratified word sorcery: covidiot, stay-safe, the new normal, build back better, the rule of six, eat out to help out, own nothing and be happy. MAINTAIN SOCIAL DISTANCE! was the ultimate expression of ancient Statecraft’s divide-and-rule policy. It is a global assault on individuality.
Function, from the individual to the State level, and everything in-between has been traumatised, transformed and subsumed. Individuals and States cede humanity and sovereignty. The private, self-elected WHO supranationalists take all. How such an unelected, illegitimate supranational, private government exists is coming under increasing scrutiny. One legal campaign lays out its thesis here.
The expression of words defamatory to government policy, even when correct, and when said or done in one’s professional opinion are no longer defensible. To professionally challenge the disinformation of government is misinformation, hate speech, and unprofessional. The punishment for stating fact, professionalism and social responsibility is censorship, mockery, a denial of expression, bank account and work. It is a civil death sentence. Murderers are punished less.
A licence to kill, not save
Never, before covid, did I believe being a State-registered and regulated physician would be a licence to peddle State delusions, death and government lies. Never would I have believed regulation would be an albatross preventing professional truth. But, this is thetruth. The last four years have been professionally difficult, for reasons comprehensively chronicled and documented. The professional regulator’s priority function is for stamping out deviance from the State narrative, and the relegation of medical ethics to preserve State control, not primarily for preservation of good medical practice.
Professional Trauma – A Hippocratic Physician in a hypocritical world
The medical profession has let the pharmaceutical fascists murder Hippocrates, and with him the profession. How does one so maladapted cope within a State system where there is no real medical alternative to The Policy, such as in the UK? Some have no need to cope, they believe the State. They believe in the State. Within the NHS, some leave, some fall ill, some are excommunicated, some lapse into denial, deceit and complicity. Some naïvely speak out, believing all that has to be done is to point out an innocent mistake of State policy to a benign, paternal government, and it will be corrected. It does not work like that. They find out. They are hounded out of house, home and profession. They are confused, and un-parented. At first, all they can do is continue to scream, professionally unheeded, and expunged. Some become pawns in politics, in a settlement to accept the damage done was wrong, but to preserve the entrenched system of lies.
Some realise this, and wonder wider: Change The System. Is this the ultimate naïvety? System change begets System. Some dream bigger: Smash The System! Is that realistic? Perhaps, the general population consciousness needs to change. Having had experience of these dynamics, I subconsciously chose a solo guerrilla campaign to meaningfully win hearts and minds, and imperceptibly swing the pendulum of consciousness. Trench warfare, small wins, seeding counter-propaganda and gently finding and supporting like-minded patients. There are no obvious kindred-spirited colleagues. The propaganda machine isolates, and foments professional paranoia. No one dares come out to another within the system. It would be suicidal. I have had one almost frank conversation with a work colleague in four years, and a handful of oblique, almost meaningless attempts to meet minds with others.
At the end of my professional Vietnam, there is a vague sense of being forever-changed, and traumatised by the system. It is hard to put a finger on it. There are feelings of surrealness, sadness, betrayal and disappointment. Of disbelief, violation, and not-belonging. It is hard to justify remaining present in it, apart from to help individual patients navigate an increasingly dysfunctional and dangerous NHS. Inevitably, there will be further assaults on medical ethics, and more tours of duty. There is no real let-up in the tyranny, only a System-pause to implement a web of control through misinformation and resource-dependency before the population may coalesce into a resistant and sentient collective consciousness.
Individual Trauma
Survivor’s guilt
There is survivor’s guilt. How come my better, braver, nobler colleagues cannot find work to make ends meet? It is not fair. I must believe some of these will thrive in some other way once they accept, like me, they have been transformed. Why should I let the system deny my fellow person a half-decent doctor? That would leave only the automatons my patients truly fear. Be true to oneself, and the whole world will change. It does not necessarily entail becoming an online persona or martyrdom. The collective Resistance has always been more than this. If enough believe and act like something is morally reprehensible, it becomes that. We have fought hard for the right to say spuriously – pretexted, fraudulent, misrepresented, dangerous, unnecessary and enforced genetically-modifyingdeathtoxin, but finally it has become a thing, if not yet a safe space.
Reboot from Within
In retrospect, for me, there has been a subconscious decision to navigate away from the NHS, but continue to practice Hippocratean medicine. I have been managing the unease by distancing and strategising. Distance geographically in rôle and in specialty. I have begun a process of retraining, re-skilling and redefinition. Of survival. A dead warrior is no warrior. A former or dead anonymous doctor of scribbles cannot even be martyred. The struggle is long, and has to be fought from within to succeed. By changing and saving hearts and minds. Let us openly state one audacious goal: infiltrate and explode the WHO from within. A long march on the institution at the heart of the profession’s cancer. Let us be aneurysmal to it. It is not entirely futile to try and survive within the system.
The function of everything, particularly in a systematised and bar-coded West: medicine, politics, law, and more seems to have been subsumed into the beast of a corrupted Big State for the sake of The State. A State for the sake of individuals, and individual agency has ceased to exist in the democratic West. Western Democracy is a political paradigm no longer seeming to work for honest, moral people. Everything about it is predicated on lies and division. The only remaining professional class is the politician: their truth is to be obeyed or one’s means to exist denied. All other professions have become politicians’ tools through regulatory commandeering and a reduction to rhetoric.
Over four years’ professional work, in multiple British general practices and international charities in Asia and Africa, my professional experience is uniformly corroborated by that of frank, international, transcontinental colleagues: no new, serious pandemic of infection. No death bug with a propensity to attack poor, coloured peoples. Only a catastrophic destruction of ethical norms, a policy and experimental gene therapy-driven mountain of death and disease, and an, “Oh why did I get that damn jab?” It makes no sense for me to believe individuals in the media or the government: they know nothing and say anything.
Coming Up for Air
There has been a longing for liberty, freedom of conscience, professional autonomy, freedom to take one’s own risks with one’s own life. I have worked in basic dictatorships where counter-revolutionaries are served drone-barbecued, but where it is still morally reprehensible to medically assault somebody, where it is still a nonsense to micromanage an individual’s every thought. I have felt happier there. I have, perversely, felt freer and safer working in an active earthquake zone and on a foreign, high altitude mountain without water, infrastructure and medical supplies than in the sophisticated perfidy of home.
It has always seemed odd that many agencies purported to be existential threats to the West cause coups in States posing a resistance to Western neocolonialism. There is at least a naïve transparency about unsophisticated States such as these. They are not pretending, and they are not trying to unsettle other States. They want the chance to be stable, self-sufficient, and self-expressed. They want an end to the barely-veiled exsanguination of wealth from within to without. I have noted in lands never colonised, the people appear more authentic, less effected, more morally-assured. Their States are unable to act as if morality is the wrong position for their subjects to adopt.
I have been quietly re-booting my medical career in a shattered and corrupt global system. The beautiful irony is here, if not in the West, one may remain human. Here, Hippocrates is not an anachronism. One may still practice professional medical autonomy and ethics working in remote, ravaged locations, developing and delivering simple medical systems and interventions to really save lives and improve health. Save a dehydrated child, a mother and newborn in childbirth, or a young adult with septic shock. Lives full of moral potential instantly and palpably saved.
None of it promotes or needs complex unquantified toxins capable of doing massive harm. Toxins easily capable of causing death seconds, minutes, days, weeks, months, and years after repetitive administration. Toxins also easily capable of being denied by a domineering State as causative of harm. These are our lives, viewed only for their usefulness in serving the system and the stock market. Anyone dispensable to the system is not worth preserving.
I have been invited to work as a volunteer in Ukraine, Moldova and in a chaotic migration centre on Lesbos. For someone with a scent for adventure, these should appeal, but I have grown tired of sustaining and serving globalist narratives. I would rather help needy nations of needy people who do not want to run away from their countries. Rather help them live better at home, independently and more healthily, but not assist organisations who thrive on disseminating and buttressing the easily soluble chaos created by a globalist system of profiteering and pseudo-culture. This system perversion means good ideas learned in the West, but no longer valued there, must be dreamt out in the East.
Collective Community Trauma
In an associate’s town where he is a senior, charitable member of the community there lies the State’s Gestapo. He has created and runs a charity. His clients are the archetypal, disempowered fodder for the State-NHS machine. One client continues to insist on wearing the same filthy and germ-ridden, four-year old N95 respirator. In covid, the State attempted to co-opt such charities to promote and propagate their covid and vaccine terror hardest amongst the most vulnerable. With this move it further enriched already-empowered, rich people. What he discloses is shocking but now normal.
There was a Council sponsored grave diggers’ initiative with the propaganda slogan: GET THE VACCINE OR MEET US!
GET THE VACCINE OR MEET US!
There was another grave-digger special, but this time sponsored by the local Professor of epidemiology, and his ‘friend’, a local religious leader whose company was said to have received a commission to deliver ‘Covid communications’. It is a sad reflection of human nature that leaders of a jab-targeted local community would squabble over funding for unethical, experimental & dangerous interventions upon themselves.
The article exhorted, Covid! Obey! There is no more space in the cemetery! The newspaper piece was anecdotal propaganda repeated by the BBC, ending with the learned article professing one month prior to the modified mRNA jabs’ rapid release: ‘Prof Wright added that the coronavirus vaccine “cannot come soon enough”.’ It is odd that such concerned pieces with such experts are not written and propagated when there continues to be a real rise in excess mortality in recent years.
The local authority militia swooped in upon another organisation: One of you is not vaxxed? Who? Why? Where? They were never told. They probed and pried, asking for the nature of community conspiracy theories and hesitancies about the covid jab amongst the staff and clients. In particular, those in the SE Asian community client groups.
FIVE TIMES the NHS sought unsolicited telephone contact with a sane, intelligent, immunocompetent stalwart of a community. It offered psychological reprogramming to help sweeten inoculation with the toxic jab.
In another locality, one State-sponsored local initiative wrote offering £500 Covid Grants-for-community-espionage:
“I would like to discuss a micro-grants scheme we can give you access to. These are up to £500 and the activities being funded must be directly related to COVID-19 either:
1) because they aim to prevent the spread of the virus, particularly by educating about how to prevent infections and the test and trace system or taking practical actions to prevent infections, or
2) funding can support groups to gather and report community intelligence and insights about COVID-19.
Insight and intelligence will inform how communications with communities should be tailored. It will also tell us more about people who are finding it difficult to cope living with COVID-19, and the reasons why.
Funding can also be used to purchase ‘capital items’, i.e. tangible objects such as leaflets, display stands, other types of equipment etc, so long as this will be directly related to preventing the spread of COVID-19 or gathering insights and intelligence.”
So much public time and money was spent gaslighting and marauding our communities for jab victims whilst the official, gathering MHRA and ONS insights and intelligence on jab damage were studiously ignored, and patients were denied access to healthcare. Our fellows continue living out and re-imposing these traumas caused by such policies.
Similar articles and projects were permeated globally. This was systematic fear-mongering designed to demand obedience with measures that were not helping them, never before implemented, nor ever proven to help them survive. Now, self-proven to harm. Experimental, arbitrary policies which replaced life-saving care with life-ending care. If they were dying more at that point (I contend, due only to policy-modulation of the unexceptional 2020 overall annual death rate) they could not die less in response to a newspaper article. They could, however, have died less if they had access to and were not discouraged from accessing healthcare, whilst being denied liberty, family, happiness and employ.
Nation State Trauma
It is of some reassurance that our State still feels it necessary to go through the pretence of goodness. It is of no comfort that all my and my colleagues’ public, unheeded but obvious warnings are, as time passes, borne out. The only thing continuing to sustain the narrative is a continuous midazolam and morphine infusion of Official Denial. Anodyne, anaesthetic, and deadly.
UK Covid Inquiry PTSD: Post traumatic State Disinformation
A further sad facet of abuse and PTSD for survivors is the re-traumatisation, and the re-living of past trauma through repeated, forced reliving of triggers, and restatements of past abuse. Hence, it was difficult to even glance at Johnson, Whitty, Cummings, et al. The conclusion the inquiry is heading to is obvious: necessary, safe and effective, and next time with faster, more draconian lockdowns. It is like an inquiry into Epstein or Saville concluding: conceal them better and supply more children, more quickly. The government concludes it did not democide us hard or fast enough.
This is the inevitable abusive conclusion about the abuse by our abusers, and our democratically elected prison guards. A faux conclusion assisted by the presence of hundreds of expensive and legal counsel paid by our taxation. A dripping roast carved from a larger dripping roast by and for a ruling class of cannibals.
The Inquiry confirms that, for the State, there is an unofficial, official unassailable evidential standard. Where criminals are convicted when proven guilty beyond reasonable doubt, governments and state-indemnified corporations operate untouchably when proven guilty beyond reasonable doubt, but within the State’s realm of implausible deniability and Policy. The UK State’s long position of permanence and power renders denial and fiction fact, and fact fiction. The Inquiry conclusively proves a State turd can be finely polished to perfection.
This State ritual of lie compaction reminded me of the then Prime Minister’s sister, Rachel Johnson. She reached out to me with a tweet on 26th November 2020. Something about what an anonymous nothing had written seemed unusually important to this clan of the system. How covid can cut both ways for this privileged sort who define our pain is troublesome. What does she really think, feel and know?
Global Trauma
Whole nations, and peoples continue to suffer the transformative trauma etched into their cultures by historic imperial and colonial policy. Globalist covid policy cuts even deeper.
This winter, the good news is the covid narrative is collapsed as a consensual idea. The bad news is the political class will never allow it to. This means our continuing misery. Statesmanship has plummeted commensurate to the State’s loss of grip on the narrative. Benevolent and moral State facades have become a thing of a by-gone age. Visible, thinly-disguised menace replaces it.
At least, for the time being, failures of war in Ukraine and approaching US-UK elections means the EU-NATO alliance cannot afford to push the weaponised pandemic narrative. So it has sought another geopolitical strategic move. Damage limitation and distraction by moving for the kill in Palestine. If dripping blood in Palestine spreads globally as did the curated lie from a wet market in Wuhan, so much the better. Losing hegemony? Just flip the script. It happened in 2001 and 2020, it happens 2024. Cycles of organised, democratic chaos. Such is the flexibility and diversity of the Killing-for-Profit model of control.
We westerners are suffering, relatively, for this killing policy. Our compliance and our vote has hitherto been bought in the 20th & 21st centuries with the wealth created by blood and oil spilled in the Middle-East, the Wild-West and the Orient. That tack no longer suffices. The protection racket built on an overstretched petrodollar is failing. Decentralised cryptos, gold-backeds and petroyuans are looming. Hence, compliance is demanded through state terror and fear. Fear of an invisible existential threat, fear of a multipolar, diverse world. Compliance through meta-fear: a social fear of not complying with the fear.
Soon State machinery will not even care to provide entertainment to distract from and conceal the multiple layering of tyranny by CBDCs and surveillance smart ghettoes. The only distraction will be fearful, endless conflict. It seems to suffice. If the US decides to avoid escalation to WW3, Russia inevitably crushes Ukraine, and by extension the will of EU-NATO. After which, the West may not only have to face up to moral and spiritual decline, but also material decline. This means hope for a return to Western individualism, and hopefully an end to American exceptionalism, for, poverty after murderous decadence could be a sobering and cathartic affair.
Change
Individuals, families, children, communities, professions, economies, and nations have been traumatised by cascaded global covid policies of nonsense percolated to humour a few and terrify the many. Internecine rifts have been riven between us. These multidimensional fault-lines fester, and might never heal in our lifetimes because community truth-telling has been politicised and censored; and because othering, cancelling and undoing is the normalised reaction to reasonable, individual thought-difference.
There is evident a neo-colonial and globalist policy of population trauma to achieve elite-sociopath agendas through physical, psychological, and pharmaceutical abuse. The abuse is multilevel and full-spectrum. It is so endemic, it has become inter-generational and inter-national in transmission. Trauma begets trauma: just read some of the 10K+ public comments below this video, it is superior to any UK Covid Inquiry, and proves the State we elect and pay believes it is there to redefine our experience of reality, and of our trauma.
Perhaps, the only positive way to deal with massive external or internal trauma is to change, not in reaction to, but in response to it. A controlled transformation with the intention not only to survive, but to surmount and succeed. To not succumb, but to reassert, whilst preserving oneself, one’s ways, and one’s mores.
It seems unreal to even think like this. It should have been a life of privilege, respect and status; not one of a fugitive in one’s country, from peers, community and profession. A pariah by dint of decency. Now is the time to make an individual stand. A quiet, firm counter-revolutionary, transformational move in a small space occupied by others. Make a small, firm personal, professional and individual contribution to counter and nullify the divisive cultural propaganda of the State.
31st January 2024
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org
Terms and conditions apply. The Covid Physician is no longer legally able to self-represent or self-identify as (still) an unheroic (NHS) medical doctor, as prescribed by law. Hence, please consider all current, past and future essays as parody, political commentary or as works of literary art by a non-medical non-doctor. This article is an artistic expression and personal view of life, should not be taken on trust, and certainly does not purport to necessarily represent the views of the medical profession or the NHS. Any patient details have been anonymised.
Denial of the magnitude of general vaccine harm and ineffectiveness is undeniably official state policy. Active harm of the population via rash, prolonged covid measures seems to be policy. The longer it is dragged out, the more undeniable it becomes.
Unsafe & Ineffective
While China and other non-Western nations purported to mete out more traditional inactivated virus vaccines, the nations of the West near-instantaneously magicked only several multi-patented genetic jabs. A mass, forced human experimentation with known inefficacy and inadequately-quantified known and unknown risks. They unleashed these upon their own un-indemnified, Western populations with impunity, whilst the West funded coronavirus gain-of-function research in Wuhan, and led with a charge of, China Virus, China Virus, China Virus. Why? Cui bono?
La pandémie? L’État? C’est WHO!
The whole system of the Western State has become unashamedly abusive and egregiously statist. Our politicians are there to be feared, not to fear us, and certainly not to represent us. We are there for them. They whom we elect and trust to represent us as intermediaries with the State. To play out their shams, to affirm the wrong they say and do to us is right. There to shield their lies, to conceal their abuse of us. In this way our State maintains itself for the sake of itself and its aggrandisement. At the same time it, as most other Nation States, is volunteering to cede its sovereignty to the WHO at the drop of a bureaucratic, self-defined hat. As long as an unelected, undemocratic, unrepresentative WHO self-identifies its pronoun with a pandemic there is seemingly one.
Pandemic Colonialism
There are two fundamental conflicts between international human rights treaties and a international global treaty of governance in a pandemic [the WHO International Health Regulations treaty (IHR)]:
(i) The IHR may suspend much of our fundamental human rights protections in favour of, for example, ‘protection of health’ or ‘prevention of spreading infectious disease’;
(ii) Human rights are based on the protection of each individual. The IHR is not. It is based on what the WHO imposes upon absolutely all of us, in the nebulous name of ‘health’ protection.
In practice this means anything the captured WHO says. In the wrong hands, such a treaty guarantees the ending of liberty for evermore on a leash of mere subjectivity, technicalities and propaganda.
The proposed fortification of the IHR married with a weakened pandemic trigger threshold, instantly and globally threatens to suspend national sovereignties and individual international human rights.
For nation States to submit themselves and their electing subjects to such pandemic colonialism is an extremely self-injurious and baffling development. Such dire international treaties are usually imposed by the victorious over defeated nations after war, or during an international bail-out of a bankrupt country.
We State subjects and sovereign individuals are thereby compelled by international law to pretend and believe a dire pandemic exists, however delusional and self-injurious that may seem. It is an entirely unacceptable but real state of affairs. It is not the way of libertarian, sovereign democratic nation States. Yet, here we are. State fodder, whose duty as State subjects is to suspend our disbelief in our nation State, in perpetuity. If one struggles to disavow one’s visceral intuition, the State prescribes Kool-Aid. An anodyne potion of propaganda to settle the queasiness, to wash the jab down. Nothing can ease the pain of being taxed into destitution to fund our harm. They have a premeditated, unproductive solution for this: Do nothing, own nothing and BE HAPPY. But, bent words are humanly unsustainable. There is a solution for this, too. Trans-humanism, or in-humanism. Your digital obedience despite State abuse is prized.
Nothing has illustrated the truth of this better than reviewing the last three years. Never has the term ‘trauma-based mind-control’ seemed so actual.
Cough Linctus
An email from the misnomered MHRA, received in March 2023, the third anniversary of the UK lockdown hammered this abuse home. These days the MHRA is a state organ self-identifying as an enabler of pharmaceutical terror rather than a watchdog against it. What was unexpected was the email revealed itself to be abjectly hypocritical, incompetent or insane. Perhaps all three. It cascaded, urgent information to all NHS clinicians, everywhere.
“Following the conclusion of a review of post-marketing safety data by the MHRA, all pholcodine-containing medicines are being recalled and withdrawn from the UK as a precaution. The Commission on Human Medicines (CHM), the independent advisory body that provides expert advice on the safety, quality and efficacy of medicines, has considered the evidence of an increased risk of the very rare event of anaphylaxis when exposed to neuromuscular blocking agents (NMBA) and advised that pholcodine-containing medicines should be withdrawn.”
MHRA, 14 March 2023
A precautionary measure detected by the allegedly world-class MHRA advanced early-warning system. Let the UK population no longer suppress any sign of the next respiratory virus pandemic, not least, its cough. Expect a Pfizer-Moderna-AZ snortable, cough-suppressing gene therapy, deliverable without consent at all crèches and shopping centres, soon. Anticipate all other highly effective, proven, safe, off-patent traditional pharmaceuticals to be disappeared.
Why so defiantly ultra-cautious, now? For two and a half years years one awaited the official MHRA alert on covid jab withdrawals. Literally from our circulations. It never occurred. Not even for AstraZeneca: that was simply suicided, honoured and shipped abroad. The irony of this ought not be lost on anyone, today. Certainly not on the relatives of the hundreds of thousands recorded by regulatory bodies as dead, and the millions ill after (or ‘with’) covid jabs, globally. But it is, and will continue to be.
In addition to Pfizer for babies, the MHRA recently announced their approval of old-variant Moderna in children, just as the WHO announces a belated end to the non-pandemic. There is no end to the serialised normalisation of MHRA madness. There is no longer even lip-service to on-the-fly, bespoke jabs for the latest variant of whatever the old variant was, to a pandemic which fizzled out years ago.
State Abuse
This kind of abuse is reminiscent of the pattern of sexual abuse and the modus operandi of its perpetrators.
The trauma of not only being traumatised, but also of it not being acknowledged. Of it not being officially recorded, or officially countered. The trauma of having to futilely recount one’s abuse so many times one gives up, more traumatised. The only treatment becomes the distraction of self-abuse or suicide. This is why many prefer a life of silence and denial.
This is why some graffiti happens. An expression of visceral pain, and social dis-ease in the face of State denial and oppression. I felt it walking home from work, my NHS sanctum of state abuse and denial. A place where, in answer to the question, ‘Would you have it, doctor?’ the phrase ‘I wouldn’t touch it with a barge pole’ is now easily accepted by a patient, when two years ago they would have reported their doctor to the police. Yet, our State persists in its fatal charade.
Secreted in the back of some alley in some unlikely idyllic, small town one finds expressions of the pain in street art. Like prehistoric cave art in blood, waiting epochs to be unearthed, decoded and understood. Cries for help from a gagged populace. A population under attack. It may as well say, ‘MHRA is a nonce’. Yes, may conclude a future archeologist, The population was under existential attack by giant reptiles and left a dying sign.
Primaeval cries for help. Somewhere, a block from a small community’s health surgery
The MHRA reminds of Sir Jimmy Savile. Both state-approved institutions for abusing public trust. Perhaps the MHRA will also take its secrets to the grave. The parallels seem more real to me. I walked the same corridors, wards and mortuaries as Savile did, at the same time as he bedazzled the public, raised money for Stoke Mandeville whilst fingering its handicapped child patients; and, as officially reported, he practised necrophilia on our dead patients. I met child social workers who all consistently said they reported such high-end abuse but were met with silence or career cul-de-sacs.
Today it is not Savile but the MHRA, and other State organs; not social workers but health-carers; not only unprotected children, but an entire, bewitched population.
Savile’s passport to abuse was lubricated by the State, multiply. The keys to a bedroom in Broadmoor high security prison with access to the Yorkshire Ripper, an unlikely passport to royalty and a BBC fiefdom replete with ample supplies of enchanted children. We remain entrapped in the grim narrative of State fairytales.
Sir Savile , National Abuser-in-Chief
WhatsApp Hancock?
Even the military style language of biowarfare and psy-ops by then UK health secretary, Matt Hancock does not raise an eyebrow in a dumbed-down population. ‘Deploy’ is not a usual medical verb. Asking, ‘When do we deploy the new variant,’ and talk of ‘frighten the pants off everyone’ is the counsel of conspiring criminals getting away with murder; not caring, concerned health ministers.
My own medical practice confirms a sense of continuous extraordinary excess death (currently 22.1% above the five-year average) and a sea of anti-coagulant prescriptions. An increased diet of atrial fibrillation, thromboemboli, cancer, inexplicable autoimmune disease, cancer, menstrual disturbance, miscarriage, stillbirths, mental illness and suicides. Neurotic children. Partners coming home to find spouses swinging from nooses. There is an unprecedented health crisis gathered.
It is now not uncommon for multiple family members across two or three generations to have died in close succession or to have suffered clots and all be on anti-coagulants. Let no one convince you this surge in sticky blood is normal or due to weather change.
There is a wilful blindness against attributing any of this to covid jabs, or the government’s destructive non-pharmaceutical measures and accelerated demolition of the NHS. A stark contrast to its active misattribution of ‘Everything by/with/because of COVID’.
NHSExodus
There is an emerging pattern of senior NHS employees, professional disillusioned, exhausted and (one hopes) morally-injured who are leaving and retiring early, en masse. There is a dangerous rise in the acceptance of remote, clinical non-contact and an inappropriate delegation of complex clinical work to the unqualified, with no time nor resources to do it. If NHS pharmacists are encouraged to practice private medicine under inadequate medical regulatory and ethical safeguards, who will concentrate on safe dispensing? Whitehall is pledging to rebuild the Promised Land, by drafting school-leaving apprentices as doctors. This is how a y vestigial resistance of professional medical ethics and standards may be completely dismantled prior to the next pandemic demolition ball. It would be unsurprising if civil servants propose drag-queens, minor attracted persons and children will be enlisted to deliver clinical care. After all, the unqualified military were drafted into conduct an unethical clinical trial. Imagine all the EDI boxes that would tick.
The NHS is, most of all, marketed these-days as a happy, inclusive shiny rainbow of robotic dancers before it is as a competent deliverer of ethical healthcare. Harm seems to correlate and be consequential to this sustained medical abuse. But no one of any authority is interested to invest in investigating this. There is only active denial and a weak misattribution of population malaise to the mirage of long-covid. Long-covid is the only voice of the covid-oppressed the State has sanctioned. The casual diagnosis hides a multitude of State sins on a sick note. Conversely, I have never professionally witnessed anyone dare offer a diagnosis of vaccine injury.
Judicial Incarceration of Free Professional Expression
Many have argued against conspiracy in covid. Some of those while arguing against the official covid narrative. Some of those say it is incompetence, not conspiracy. Some say all this whilst retaining anonymity. Surely, it is evidence of conspiracy itself when one fears retribution in exercising legal free speech?
The disturbing fact is that since Dr Mohammad Adil’s unsuccessful High Court appeal judgment, even this blog is not legal free speech within the parameters ‘prescribed by law’ through the GMC’s updated social media guidance. This judgment may have imperilled all the country’s professional classes to the mercy of arbitrary, illegal, and unprofessional lawmaking professional regulatory bodies, depending on each’s under-pinning primary legislation. One hopes incognito lawyers, such as The Secret Barrister may be anxiously blogging and advocating for Mr Adil and fellow anonymous professional bloggers’ fundamental legal rights.
The judge has, in my analysis, extraordinarily concluded that anything the GMC recommends is ‘prescribed by law’. If one accepts that the primary legislature is Parliament and the only secondary legislator is the Executive, how can the GMC be held legally tantamount to the Executive as a de facto, unilateral prescriber of law? It cannot even be trusted to uphold medical ethics. The GMC is now endowed with both the magical power of being the mind of the public and the legislator. The judgment seems a fallacious, circular construction of extreme judicial convenience made in obeisance to the State tyranny. It is certainly no way of checks and balances to GMC-MPTS overreach. Dr Adil plans to appeal.
May I appeal for readers to bring urgent attention and prayers to Dr Bhakdi’s case. It is another example of intimidating eminent medical experts from professional expression. Not a more gentle, peaceful, caring and morally-courageous colleague have I ever come across. He is a touchstone for world truth in covid. He is being persecuted, and inappropriately prosecuted without proportionate justification in a German court. This distortion of his intent is symbolic of the evil he is fighting. Germany is creating inter-sectional hate by abusing its laws.
This is the strange equality of our current State constitution. An abrogation of national sovereignty, industrialised denial of abuse and a crude, inclusive, global equality of maximal outcome regardless of competence, unequal speech, unequal opportunity, unequal standards of judgment and disproportionate measures. The sole MP (the heroicAndrew Bridgen) dropping the truth bombs reflecting my and my patient’s last three years within medical practice was expelled from the Conservative party. The Labour government-in-waiting are worse for not offering any fair counter-representation of those many in their constituencies suffering from government covid policy.
There is no doubt there are conspiracies. Events and words, things said and done, and not said and done, all glued together by an unbelievable global synchronicity and similarity. Agreement is a matter of degree and a matter of time. The worst case scenarios seem to be playing out incrementally and imperceptibly. On a micro (my own professional concerns and experience) and macro level (official statistics, my censored peers and their larger studies). Only the Pharma’s brief, flawed studies which will never be required to be scientifically verified are either heard or allowed to be redacted and buried. Honest professional experience beats the dishonest RCT in an evidential hierarchy on pharmaceutical safety.
There are conspiracies to make as much money as possible with the least financial risk. Conspiracies to mislead. Conspiracies to deny the facts, deny harms and deny alternative, valid narratives. Conspiracies to compel, force and scare. Conspiracies to engineer and fabricate a noxious gene sequence to go severally into each and every arm. What remains to be confirmed is a conspiracy to kill, to harm, to eugenics, toward a centralised global tyranny (benevolent, of course), an illegitimate world government elected by fear, sustained by perpetual emergency and held together by a WHO constitution enshrined in international law.
18th May 2023
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org
The Covid Physician is no longer legally able to claim to (still) be an unheroic NHS doctor, as prescribed by law.
This article is a personal view, should not be taken on trust, and certainly does not purport to necessarily represent the views of the medical profession more widely or the NHS. Any patient details have been anonymised.
Medical Ethics & Free Speech are under fatal assault by an unassailable military–pharmaceutical cult profiteering from the cultivated terror of death
GMC: Government or General Medical Council?
There is a pogrom of ethical doctors in the West’s formerly democratic, once Free World. The UK is an exemplar.
Wrongly pursuing ethically-minded, safe, caring doctors via unreasonable GMC investigational and prosecution procedure is destroying the UK profession’s ethical foundations. The GMC’s criteria for acceptable, professional medical opinion seem arbitrary, subjective and politically motivated. At times, it behaves manifestly illegally. The legal uncertainty engendered by such GMC misconduct is compounded by ‘overarching criteria’ of the Medical Act 1983. These are being misapplied resulting in suppressed professional medical free speech. This is damaging public confidence, public health and professional medical standards. Urgent reform of the GMC legal test of professional medical free speech is required to reflect fundamental rights and prevent the GMC misapplication of medical ethics to, in fact, destroy professional medical ethics and the public health. Medical workplaces, and indeed fellow colleagues are increasingly moving to arbitrarily suppress and control dissenting doctors’ free speech. Ofcom’s political remit to curate the country’s official covid narrative has institutionalised the illegal restrictions on general and professional medical freedom of expression. GMC guidance to prevent anonymous, legal professional medical free speech made precisely in the interest of the public health is further indicative of a loss GMC regulatory compass and competence.
Time is proving persecuted dissenting doctors right. The state did not protect us, the MHRA Chair has relinquished its function to ‘stop the (government) killing people’. It should not be right in a moral, ethical society for individual, insightful brave doctors who point out the obvious damage of state non-pharmaceutical and pharmaceutical measures to be subject to abuse by their regulatory body. Nothing will change in the future unless there is sweeping institutional and political reform. It will only get worse. By trying to remain politically legitimate the GMC has lost any legitimacy to regulate ethical doctors.
The widespread persecution of doctors and medical ethics is sudden, simultaneous and global. It appears to be a systemic, coordinated phenomenon. Finger-pointing to individual doctors is missing the point. Internationally, vocal doctors who speak their inconvenient truths, are ruined with a sophisticated, pre-planned and propagandised intent to maintain an unassailable, fatal covid vaccine narrative. Western medical regulators are mis-regulating with the tools of intimidation and fear. Principally by destroying individual, exemplary medical professional reputations without respect to any moral, legal or ethical principle. In a sense, these medical regulators are not concerned with maintaining high ethical standards in the profession. Contrarily, in the last three years they have been trampling on them in favour of suppressing intelligent, ethical, and life-saving medical counter-propaganda. The regulators must be stopped.
I will discuss the persecution (calling it ‘cancelling’ is inappropriately mild) of some of these fine doctors, and conclude by examining why this occurs and what may be done to end it.
The GMC legal standard to which a UK doctor is governed
Medical Act 1983, section 1. The affliction at the heart of medical ethics
1 The General Medical Council.
(1)(1A)The over-arching objective of the General Council in exercising their functions is the protection of the public.
(1B)The pursuit by the General Council of their over-arching objective involves the pursuit of the following objectives—
(a) to protect, promote and maintain the health, safety and well-being of the public,
(b) to promote and maintain public confidence in the medical profession, and
(c) to promote and maintain proper professional standards and conduct for members of that profession.
These functions only allude to something else other than the above 3 core values. They relate to a more fundamental professional medical ethics. These ethics are unsurprisingly constant and timeless. Ethics appear to have become less important and operative in the mind of the GMC and MPTS(The Medical Practitioners Tribunal Service), and taken an inferior position to their prescriptive ‘proper professional standards and conduct’. So have basic, natural legal rights: in a rudimentary failure of law and legal process the tribunal Legally Qualified Chair and GMC counsel overlooked the right to basic legal free speech of Dr Sam White. Why? Because their focus was incorrectly on the Medical Act 1983, secondary prescriptive rules of GMC formulation, and politics, not medical ethics. This shift away from fundamental professional ethical values seems more evident since the era of Dr Shipman, and the move of the GMC to appease the government, so as to preserve its regulatory position at the expense of medical ethics.
How does the GMC objectively determine the health, safety and well-being of the public? Judging from March 2020 onwards, I would say it does not. It is subjective, based on contemporaneous political expediencies and the prevailing propaganda.
How does the GMC objectively determine the undermining ofpublic confidence in the medical profession? I would submit it may be based subjectively on political correctness and prevailing propaganda rather than a true delve into the collective mind of the public.
How does the GMC objectively determine proper professional standards and conduct? I would suggest this is based not as it should be on debating of the scientific paradigm, real clinical experience and ethics to refine them, but subjectively on politics, and the corporate capture of scientific institutions, individuals, pharmaceutical guidelines and journals.
Caution should be applied in interpreting the meaning of ‘the public’. First, it should not be conflated with ‘the public health.’ This is a very different and political beast. Some might say public health has nothing to do with the public or health, but everything to do with subverting human norms for political tyranny and corporate profit. Second, it cannot be presumed that the GMC, the MPTS nor the Judiciary necessarily interprets ‘the public’ as either meaning the individual ‘patient,’ or ‘patients’ as a whole. Dr White’s and Dr Adil’s cases (discussed later) illustrate, I suggest, a contrary tendency.
His recent GMC tribunal transcript may be accessed here, or here. Around April 2020, Dr Adil made a prescient and prophetic calling out of the crime of crimes: a global lockstep lockdown and coercion toward mass human biological assault. He scientifically questioned the existence of SARS-CoV-2. It remains difficult to call state-funded, premeditated genetic engineering and wilful pharmaceutical ignorance of basic science either ‘experimental’ or ‘accidental’. If one still remains unconvinced by these concerns, this presentation by Professor Denis Rancourt of the hard all-cause mortality data of the last three years may assist. It is as shocking as it is compelling: in summary, no viral respiratory infection pandemic, democide by policy, and cumulative pandemic by serial covid jabs.
Dr Adil’s alleged professional misconduct is predicated on the GMC’s subjective view of what the prevailing attitudes of a gaslit UK public and UK medical profession were in April 2020. Those attitudes were engineered by censorship and the sophisticated psychological and political propaganda of 2020. It is not interested in what Dr Aseem Malhotra (see below) is getting away with saying now, in 2023. By this reckoning, even if Gates, Tedros, Whitty and Hancock were hanged at Nuremberg 2027, the GMC would maintain Dr Adil could not possibly have known in 2020, and it would still destroy him.
The GMC believes Dr Adil’s words were more terrible because he promoted them with his professional credentials and seniority. This is perverse reasoning by the GMC tribunal. On the contrary, more credence should have been given to his words because of his professional medical status. Look towards politicians and philanthropists for medical wisdom is recent fashion.
Thank God for the trail-blazing Dr Adil. His was courageous political and scientific dissent, which should not be suppressed nor need to respect majority professional or public opinion and feelings. His ethics are sound, but his views were rendered apparently fringe. Not anymore. Even so, this does not make them professionally, scientifically or politically irrelevant or wrong. The GMC do not care if time vindicated him. It says it was wrong in the context of April 2020. That, is equally perverse. Basic medical ethics ought to be immutable and independent of time, fashions and psychological onslaught.
I quote some of the extraordinary travesty in the tribunal proceedings:
54. In the context of the pandemic at the time, and particularly the concerns of a public confined to home and dependent upon the provision of responsible and trustworthy information, the Tribunal’s view was that such statements, containing mis-information and conspiracy theories, could be both confusing and destabilising. They had been made by a senior UK surgeon with many years’ experience in the NHS. In addition, Mr Adil had promoted his professional experience and credentials in the videos so as to engender trust and confidence in their content in the minds of his audience. The Tribunal determined that, it was more likely than not, such comments undermined public confidence in the medical profession.
83. … The GMC acknowledged that the comments set out in charge 2g were made before any vaccine had been developed, but the comments were lurid and unconscionable and undermined the vaccine programme then in development, which has since proved to be the best way through the pandemic.
84. Mr Kitching submitted that Mr Adil appeared to be finally gaininginsight but it was new insight and far from complete. To a degree, the developing insight reduced the risk of repetition but Mr Adil lacked widerinsight and that was the concern, and therefore his fitness to practise was currently impaired.
Dr Adil’s GMC-alleged conspiracy theories and misinformation have now entered Hansard, and one of those responsible MPs, Andrew Bridgen has now suffered a thinly-veiled witch-hunt of his own. He is expelled from his own party, whilst the feckless, equally-expelled ex-Tory, and former Health Secretary, Matt Hancock has so little insight he calls the quoting of properly contextualised covid vaccine scientific statements, anti-semitic. It is the most odious technique of censorship, practised by a miscreant in public office. For Hancock, Bridgen is an existential threat. Bridgen now sues Hancock for defamation. Whilst all is collapsing around Hancock, he remains defiantly sociopathic. As usual, his desperate, divisive and vicious rhetoric clings to the false narrative he created and maintains three years on, only with UK excess deaths at record and rising levels exactly because of Hancock. In the inflated pretence of saving the few, Hancock killed far more.
If Drs Adil and White were also MPs, or Andrew Bridgen, MP also a registered medical practitioner what would the GMC feel was right to do? Would it avoid them because they were also practising politics? Would it leave the persecution to parliament? Why should that make all the difference?
Time and Tavistock
Will the GMC pursue the doctors at the Tavistock clinic now there is some perceived furore against their possible professionally-abusive conduct toward children? Did they or did they not in the recent past do things professionally to offend the overarching objective of the GMC as enshrined by the Medical Act 1983?
Does the apparent GMC standard of ‘the prevailing, publicly fashionable view’ of medicine applied in Dr Adil’s case apply to the Tavistock doctors? Probably, but only because as a matter of political convenience it helps the GMC politically persecute Mr Adil, and avoid scrutinising the, (dare I say ‘woke-ified’?) Tavistock medical teams.
Times change rapidly, but, medical ethics should not. These ethics are not civil laws that may be legislated on political whim in parliament. Murder is a still a crime because it is, at its essence, immoral, not because a judge or politician says so. Not acting in the best interests of patients (one unreliably presumes these patients are ‘the public’ which the GMC has a legal duty to protect) is professional misconduct because it is essentially unethical, not because the GMC says it is misconduct at only certain points in political time and space, for only certain doctors.
It may be that the majority of the UK medical profession and public did not and do not accept a political, corporate-sponsored ideological game of the hormonal or surgical destruction of a child’s biological sex and gender. It may be that, due to an unrelenting diet of well co-ordinated minority activism and sophisticated propaganda, no one dared to protect these poor children at the time. Dr Adil did not commit this error when he sought to do his professional, ethical medical duty of protecting the public when he voiced his serious and time-vindicated concerns.
Forcing state compliance with an unacceptable minority and/or extreme medical ideology upon professionals, adults and their children is something the Government, Tavistock and the GMC may have in common (future GMC counsel please note: this is my current reasoned hypothesis and opinion – not past or future conspiracy theory or misinformation).
Dr Adil v GMC, High Court, February 2023
Dr Adil made a reasonable statement updating and briefing his position on 15.10.22 His case is listed in the High Court for February 2023. It is a watershed moment for my profession. The profession has a duty to support his right to a freedom to express a professional opinion. It is not a matter of whether one likes him or how, what, nor even primarily about why he speaks. It is that he should not be made to feel he can’t speak. It is a pivotal matter for doctor, patient and the public health.
The High Court judgment may not be personally favourable to Dr Adil. If it is not, it must be hoped it will favour the medical freedom of expression for the profession. Being outspoken should not be medical misconduct. His conduct represents the best of strong, ethical and intuitive medical ethics. His overriding and unbearable concern for patient safety and ethics is not good enough for the GMC. Neither is his being ahead of his time, nor his being a proponent of legal, medical free speech.
His primary risk to the state is his senior status and his opinion, neither of which are risky or illegal. This letter from a fellow surgeon seemed fair and reasonable on 13th July 2020, but time has shown Mr Adil to have not in any sense been fantastic at all. He has being excluded from medical practice for three years because of his political and scientific beliefs and opinions at a point in time, not for medical incompetency. He may not be the slickest social media operator, nor the most skilful public advocate. These are not of his professional skillset. He is a good doctor who did his ethical and moral professional duty in a timely and effective manner. He is guilty only of placing his professional concerns about patients’ welfare, society and public health above his own and his family’s welfare.
One of the unspoken issues about Mr Adil is he is a victim of his time. He is an old-school surgeon and doctor. He is a child of his generation. He is an anachronism of high professional morals and ethics. Independent, and fiercely protective of his patients, not himself. No one seems to value seniority and professional competence anymore. What matters is political compliance. Give my patients an ethical, independent, competent senior doctor any day. It is precisely what society, public and each individual patient is desperate for.
GMC-MPTS Institutional Bias
Dr Adil’s powers of linguistic finesse on complex sociopolitical matters in the public domain may have done him an injustice which the GMC fails to recognise. It seems an obvious point. Mr Adil seemed largely self-represented until latterly, and under severe professional, financial and public stress. It is no coincidence the Mr Adil has recently highlighted the high death and suicide rates of doctors undergoing GMC scrutiny.
He draws attention to genuine and judicially proven concerns of institutional racial and cultural bias in the GMC-MPTS process. It is not merely proven racial inequality. It is proven GMC race discrimination. Take the case of a mixed race, African and muslim NHS Surgeon. Dr Omer Karim’s solicitors say he ‘was a whistle-blower about patient care and raised concerns that ethnic minority doctors were being subjected to bullying’. He somehow ended up with GMC professional misconduct charges, and the GMC was somehow found guilty of race discrimination on appeal at the Employment Tribunal.
The GMC planned in 2021 to appeal that decision. The BMA pledged to support Dr Karim in any further appeal. His case is a landmark not only for the proven racial discrimination against the GMC, but for also being procedurally decided at Employment Tribunal with the GMC regulator positioned as his de factoracist employer. The ET made three key conclusions:
At para 106, (1) “BME doctors are more likely to be referred to the GMC for fitness to practise concerns than their peers and are more likely to be investigated by the GMC and, ultimately, to receive a sanction.
(2) “The Tribunal was concerned that there was, in our view, a level of complacency about the operation of discrimination in the work of GMC or that there might be discrimination infecting the referral process.”
and at para 108, (3) “We have come to the conclusion that there is a difference in the treatment of the Claimant in contrast to Mr L, a white doctor. We do not consider that there has been a credible explanation for the difference in the treatment.”
Part of Dr Adil’s personal concerns of racism in his case may also represent an equally unacceptable cultural bias by the GMC against Mr Adil. He is not only the product of being originally from a different country but also a different generational, religious, moral and ethical milieu. These are not impairments, and may even be assets. In a time of faux wokeness it seems more unjust for these real cultural, language and stress factors not to be taken into account in the impending High Court decision.
The reality is we have a skilled, senior, caring surgeon being excluded from giving to our society and being denied a vocation and living. He is deskilling. Even though he has accepted to the tribunal that he was wrong in much of what he said, much of it was not and is not wrong. What this noble doctor lacks in culturally acceptable style he overcompensates for with immense professional substance. This individual professional competence is his real offence to the politicised medical regulatory system.
Mr Adil cannot diminish the public confidence, public health of the profession by a minority and diverse opinion. He can only enrich or correct it. It is not a case of a rotten apple corrupting the barrel. He is not rotten. Nor is it the case, as the GMC counsel suggested, “whilst it was not akin to falsely shouting ‘fire’ in a crowded theatre, it was not far short of that”. Shouting ‘fire’ and causing public pandemonium by fomenting population fear, anxiety and panic is precisely what the WHO and most governments so callously did for an infection fatality rate which at its known worst was in the order of flu, or much less, with an average age of mortality curiously similar to average life expectancy. In April 2020, Mr Adil was a lone voice of reason in a global storm trying to temper the madness. For that, it is the WHO and our government that should be brought down, not Mr Adil.
The only way for Mr Adil to survive is if he has money (please donate to his crowd-funding page) for effective legal representation, the court find in favour of his legal free speech, or if he submits himself to a humiliating GMC brainwashing programme to correct his inapparent, poor professional insight. He has been more professionally insightful than any of us. His primary failure in insight was to believe the state and the GMC would allow and respect him to speak his professional concerns commensurate to his seniority and long medical experience.
There are many examples of favoured media doctors being way off the mark in regard to the science, vaccine effectiveness and safety who were left alone, or have slid away quietly, their bank balances fortified and their burgeoning professional reputations intact. They were left alone by the GMC and permitted to be unprofessional, unethical, wrong, dangerous to the public because it suited the propaganda of Ofcom and its government.
Our society is very confused. Mr Adil deserves to be honoured as a pioneer and medical hero. He is not, because he lives in a time of communist and corporate fascist tyranny. It is a world of lucre with no place for liberty, morality nor ethics.
Dr Adil and Dr Kayat, poles apart on the spectra of clinical experience, ethics, media attention and GMC scrutiny. Only Dr Adil has been, and remains, suspended over three years. Source: video
Dr Sam White, General Practitioner
Dr Sam White was also an early medical martyr. His individual courage and belief gives doctors some hope. He voiced reasonable concerns about vaccines on social media. The GMC moved, illegally, to stop him. The High Court simply pointed out the obvious, asking: Why were the GMC illegally restricting his freedom of expression? GMC counsel, the Legally Qualified Chair and his own representation had overlooked this. Perhaps because the propaganda machine was so intensely febrile with covid psychosis. More extraordinary was a rapid communication he received from an NHS England representatives who illegally and summarily informed he could no longer work anywhere in the NHS. It was for him to prove both these decisions were grossly arbitrary and illegal rather than those political minions to know it. These are abuses of power.
It is accepted that Mr Adil’s comments were in some degree speculative, and hypotheses based on circumstantial evidence. Equally, there was primary evidence present which he would have had access to so as to bolster his opinion. However, Dr White’s case proves that even evidence-based comments are not enough.
This is what got Mr Malik into hot water.That two workplaces should simultaneously move to quash his free speech for his echoing of a parliamentary debate on vaccine safety by asking him to remove his social media post is of public and professional concern to us all. Even if the GMC dare not tread on him due to the ‘current context’, his two workplaces do. Mr Ahmad, I believe is working in the private sector. I speculate that the two companies will say that he does not share their commercial values. However, legal free speech medical ethics, and acting on well-founded, serious concerns should be shared and celebrated by his host companies. They should gave him an award, and say his conduct is exemplary. They should line the corridors, dance and clap for him and all ethical doctors. They should positively discriminate and employ more doctors like him. Mr Malik also stood up for us all in January 2022 when he defended bodily autonomy and spoke publicly against mandated biological, experimental gene therapy to remain working in the NHS. Why did his workplaces not choose to persecute him, then? His responsible, ethical and refreshing response to tyranny proves the adage the only remedy for suppression of freedom of conscience and expression is more free expression.
Mr Ahmad needs surgical theatres and a complex team to operate, he is more dependent on business forces. It is harder for him to set up alone. It is not extraordinary to say that his workplaces may have financial conflicts of interests in regard to their personal, political and business connections with individuals and companies which induce them to harm him.
Dr Aseem Malhotra
Double-jabbed Dr Aseem Malhotra is equally courageous. However, perhaps, at least in his non-interventional cardiologist private practice, he is less susceptible to commercial prejudice and bullying. That being said, what if his publisher, or a leaser of private rooms wrote to him announcing that his strong sense of medical free speech and medical ethics were not values they shared. If that did happen, it would be a medical cancelling reminiscent of JK Rowling’s (TERF) persecution for legal free speech in defence of women.
Dr Malhotra published to Twitter these remarks purported to be made by the GMC following his being predictably politically whistle-blown to the GMC:
What is clear from the GMC comments on Dr Malhotra’s case, is the GMC was a keystone in the political, state plot to bamboozle and menace the public into obviously rushed, risky, ineffective, experimental and misrepresented gene therapies.
It is disturbing when the GMC deals with well-founded and serious professional concerns with nebulous disinformation terminology such as ‘conspiracy theory’ and ‘misinformation’ while itconspires to misinform the public in league with the government and Ofcom.
Although Dr Malhotra may have viewed his sparing as a huge victory, it seems not to me. The GMC’s selective sparing of him creates no legal precedent for the rest of us. It is a tactical withdrawal decision by the GMC. The GMC seems to be saying they may, depending on political expediencynot persecute a Dr White, Ahmad or Malhotra once the job of delivering the bulk of experimental, multiple jabs is done, but they will continue to persecute Mr Adil, and not Dr Kayat, nor her ilk. This is very concerning. It gives no legal certainty to doctors, leaves the door open to more arbitrary GMC behaviour and self-endorses the charge against the GMC that it holds a constant, unpredictable and prejudiced threat over doctors’ professional heads. This is no way to regulate but every way to intimidate. It destroys and controls doctors for political imperatives, and not in any way for individual or public health.
Candour, Consent, Whistleblowing, Free Speech & Privacy – The Unsquareable GMC Circle
GMC social media guidance
Not only is the GMC illegally regulating doctors ECHR article 10 rights, it is recommending doctors forgo their article 8 rights to privacy. At the same time it stipulates professional duties of candour and informed consent. How does the GMC square such circular legal contradictions? By illegality and selective, prejudicial, political persecution of scapegoats.
The GMC has produced social mediaguidance for doctors. This reveals the GMC not only antagonises reasonable, self-declared whistleblowers, it also has no approval for anonymous medical whistleblowers and writers on social media. Its social media guidance to doctors recommends that it is done without the privilege of anonymity.
I have written on covid, the plight of dissident doctors and the uneven hand of the GMC, before. Does political or professional criticism of the state and GMC reduce or increase public confidence in the medical profession? Should I be writing this? I have no doubt it is legal, but is it professional? I believe it is for the reasons, herein. Particularly, as it is supported by true professional experience, reason, examples and evidence. It is also journalistic, opinionated and sometimes utilises the literary device of humour. Is that wrong for a doctor? No, there are many doctors who do this all the time. They are never pursued by the GMC. It is not necessarily because they are any more or less. It is simply because the GMC politically determines what it believes should be in the public confidence and of a professional standard, based primarily on the grounds of what it subjectively believes is within the acceptable window of current political discourse and public opinion.
I make clear my views are not those of my employers. By my anonymity I protect my patients’ identities, my employers’ feelings and my right to professional, personal, journalistic and artistic freedom of expression and conscience. One has to accept as an anonymous whistleblower what is lost in professional credibility is gained in an exercise of the GMC professional duty of candour without incurring the unethical threat of persecution by the GMC. It is therefore confused and perverse of the GMC to (correctly) conclude:
‘They (doctors) must support and encourage each other to be open and honest, and not stop someone from raising concerns.’
Why, then, does the GMC obstruct and not lead the way?
It is relevant to state I am a doctor and necessary to remain anonymous if I am to contribute to the professional and societal debate with an equal right to anyone else in our society. It is in the interest of public health, public confidence, democracy, patient safety and our profession. Most particularly, because the government, and the state system of regulation and safety (parliament, MHRA, GMC, PHE, UKHSA, ONS etc) and our media have failed to protect and inform the public. Where was the GMC on vaccine informed consent, unethical experimentation, and vaccine risk-benefits?
Where was it to regulate Drs Chris Whitty and June Raine and so forth? Unfortunately for justice, the High Court has ruled there are doctors with a “sufficiently close link with the profession of medicine” and other doctors’ functions which are “too remote from the practice of medicine” to be subjected to the GMC’s standards. This alone gives the GMC sufficient cognitive wriggle room to turn away its attention when politically expedient.
There is a mismatch between theoretical whistleblowing policy, hollow public body statements on paramount patient safety as compared with the reality of GMC scapegoating of individual, ethical whistle-blowing doctors. The GMC’s social media guidance compounds the mismatch. If there are public interest grounds to allow anonymous whistle-blowing of doctors to the GMC, shouldn’t the same argument apply to whistleblowing medical free speech?
In September 2022 it was reported Professor Karol Sikora was being investigated by the GMC, but it would not tell him why. Up until that point, Professor Sikora has been a constant, reasoned and strong public voice critical of the government’s covid measures.
The Governance of the GMC
Unfit for Purpose
After the bizarre and selective persecutory pursuit of Dr Manjula Aurora, fellow doctors have labelled the GMC unfit for purpose and self-serving. The GMC is not just extraordinary for simple doctor-bashing. Once, the GMC-MPTS process did not sanction a doctor at all for one of the greatest medical sins: sexual relationship with patient. In this 2016 case of Dr John Brookes, the disgraceful message and excuse was given that a surgeon with magic fingers is too uniquely-skilled to take out of the NHS. What about the ethical doctors taken out of the NHS by the unethical GMC covid pogrom? Politics matter to the GMC-MPTS process. Morals do not matter, ethics increasingly do not, and the Medical Act 1983 is subjectively and politically interpreted by the GMC and the Tribunal for their own conveniences. The process has become a corrupt inversion of itself through self-interested preservationism and political sycophancy.
The Tyranny of Dogma
The trouble with GMC medical regulation is rather like the trouble with medical science. Politics, regulation of doctors, medical scientific research and profit have fused into a dysfunctional mutant causing pandemics of technocratic kleptocracy and iatrogenic illnesses. Dr David Rasnick’sessay on the tyranny of dogma explains this.
GMC Institutional Dysfunction
Why does the GMC conduct itself in an inconsistent, illegal and unethical manner? One reason is the institutionalised legal laziness and legal over-reach informed by a sense of untouchability as in the case of GMC Counsel and the Legally Qualified Chair missing the overriding and simple matter of Dr Sam White’s article 10 freedom of expression rights.
A second is the GMC-MPTS quasi-judicial process of tribunal decision-making does not set internal precedent. What goes for one doctor, does not for another. The precedent is made in the High Court and requires endless money, and resilience. Many doctors who feel aggrieved therefore capitulate to, and accept the injustice, blame, and humiliation. They pay lip-service to the probational behavioural modification and re-programming just so they can avoid bankruptcy and the suicide-inducing stress of a prolonged suspension, loss of vocation, home and livelihood.
A third is the GMC’s dysfunctional guiding legislation. This can only be corrected by a careful, responsible revision of the Medical Act 1983. Unfortunately, any redrafting by woke 21st century legislators may only make matters worse.
A fourth is politics.
The Privy Council
A fifth issue is the GMCs legal personality is granted through Royal Charter by the Privy Council. The GMC Council is composed of 5 medical professionals and 5 lay members. The appointments process is described as ‘following an independent appointments process.’ All members are appointed by the Privy Council, including the new, current Chair. This is a body arguably even less democratic, more opaque, powerful and less accountable than parliament. The GMC’s power to make regulations, under the enabling Medical Act 1983, with respect to the medical register can only come into force when approved by order of the Privy Council. These factors represents another political conflict of interest grating against patient health and the preservation of the core professional ethical values of the doctor-patient relationship.
The GMC was politically compelled to reform after the Shipman Inquiry, 2004, and under some threat of losing its regulatory relevance and status. The essential concerns were of a GMC over-focused on professional interests, rather than patient interests. It is debatable this reform has only created a politically-captured medical regulator more interested in being politically correct than being ethically correct. Thus, through its recent weaponisation by government covid policy, the GMC is in more danger of becoming increasingly and irrevocably illegitimate in the eyes of doctors, patients and ‘the public’. It was Sir Graeme Catto, then GMC president (not Chair), who said in 2006: “Modern medical regulation must put patient safety first.” Indeed it should.
GMC: Reformation or Destruction?
The GMC has become a political sword against ethical doctors and is not an effective shield for patients, ethics, the public confidence nor public health. Why should we doctors pay the GMC to misconduct itself and in doing so, drive the standing of our profession into the ground?
The GMC is desperately in need of meaningful and constructive change. It cannot continue to be allowed to flagellate or muzzle ethical doctors with impunity and disregard for their fundamental legal rights or the medical ethics which it may purport to guard. Dr White’s case and Mr Adil’s upcoming case, even if wholly favourable to medical free speech, are only sticking plasters.
The cancellation of good doctors (or any other good health carer) for no good or legal reason is now a real phenomenon and pernicious to our society. Any system supporting or encouraging such an act is cutting off the nose of society in spite of society.
The GMC has a duty to demonstrate insight. The GMC must recognise that non-propagandised, non-censored professional medical free speech is healthy and commensurate to the number of professionals sharing the message of that speech. It is not a case that one experienced doctor speaking within a minority or at one pole of a spectrum is necessarily wrong, a danger, unprofessional or unworthy of being heard. Not even in the time of global social media, but particularly in the time of global social media.
Meanwhile, as the GMC continues to serve politicians while it bullies medics into practicing defensive and obedient, corporate-captured medicine, and drives doctors to their deaths; our patients continue to increasingly die in across age groups, globally and in the UK (as I reported and predicted).
What majority of doctors is going to suggest it is due to modified mRNA population experiment when the GMC is rabid guard-dog to the government’s impossible ‘safe and effective’ mantra? Without the GMC’s misguided stewardship and cronyism, there is every chance the profession would have swiftly realised the public truth of the unethical, unsafe and ineffective experimental biological interventions two years ago, and actually prevented deaths.
Sent 25.1.23. Patronising misinformation and programmed, wilful institutional helplessness. The GMC is co-architect and co-conspirator in the demise of ethical professional medical practice, the collapse of the NHS and the nation’s ill health. Its Chair does not seem to know. She does not seem to realise she does hold the ‘magic switch’: with it she must stop GMC persecution, protect and not undermine our professional mores and ethics, stop GMC cultural and race prejudice, and stop politically policing doctors’ legal, professional free speech.
A Western spiritual and intellectual crisis
Other professions and professional regulators are behaving politically
Lois Bayliss, solicitor, helped countless individuals in a David versus Goliath battle against the covid narrative. She is now being pursued by her regulatory body. A UK Magistrate was sacked for using her suffix “JP” in a request for ICC to investigate crimes against humanity. Popular political commentator, Dr Jordan Peterson, who incidentally happens to be a gifted psychologist, is politically attacked by his professional regulator, the College of Psychologists of Ontario. It should have more psychological insight into how it politically abuses it position, and into how psychologically abusive it is to suggest one of its foremost psychologists should be politically reprogrammed. There is a full spectrum attack on professionally laudable, moral, ethical and legal free speech.
Religion
It is not just Western morals, ethics and human rights under persecution by Western institutions. It is the deliberate self-harm of their historical basis, Judaeo-Christian thought. In November 2022, a peaceful woman, Isabel Vaughan-Spruce was arrested by British police in violation a local council ‘censorship zone’ for a crime against natural human existence and potential thought. She was standing silently in public, and possibly praying in her head outside a closed abortion clinic. Compare this with the complicity of the police in the mass violation of bodily autonomy perpetrated by the government and GMC in the name of Pharma and covid vaccines. Her case goes on trial February 2nd 2023. All religious people should support her. Particularly muslims, whose religious freedoms and similarly conservative beliefs are selectively tolerated in the West, while the West does a demolition job on its own. For, Western censorship of religious free thought, conscience and speech will, one by one, come for all religions. This, as Scottish police are permissive to paedophilia by euphemistically discussing them as MAPS, ‘minor-attracted people’.
The fundamental tenet of medicine, primum non nocere – first do no harm has been inverted. It is not merely the case that it has been ignored. Government and GMC policy is obviously and actively democidal. They did not exercise any precautionary principle – this required evidence of no harm, and significant benefit. There wasn’t any for their non-pharmaceutical or pharmaceutical interventions. Coercing, forcing and inducing every person in the world to playing unnecessary pharmaceutical Russian roulette is not the precautionary principle. The GMC would do well to heed both Hippocrates, and Laozi, since, the fundamental Taoist principle of wu wei – action through non-action is very Hippocratic, and apposite for our headless, heedless times. Had the government and the GMC simply done nothing they would not have harmed and killed so very many, and saved so very few, if any.
“I believe that political correctness can be a form of linguistic fascism, and it sends shivers down the spine of my generation who went to war against fascism.”
Amidst today’s centralised reprogramming of the meaning of fundamental words such as ‘woman,’ ‘pandemic,’ ‘menstruation’ and ‘vaccine;’ and the career-ending, international prohibition on the truthful juxtaposition of the words unsafe, ineffective and ‘vaccine’ we must also add global linguistic-communism to the lexicon. What would she have made of that?
With regard to past and present medical regulator approved communo-fascist medical tyranny, The GMC has responsibility for encouraging this type of extreme political climate of fear around freedom of expression and conscience. This fear was heightened in covid. To the extent where a publisher broke off relations in 2021 when I refused its request to self-censor these parallels of our covid state with fascism and Nazism. I had been writing of the parallels since 2020, here, here, here, and here. I had never imagined the UK had sunk so low. To Vera Sharav, and other Holocaust survivors who have witnessed it all before, I will leave the last wise words.
31st January 2023
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org
The Covid Physician is (still) an unheroic NHS doctor. This article is a personal view and does not necessarily represent the views of the NHS. Patient details have been anonymised.
Complicit Chess Pieces in an Elite-Orchestrated Class Warfare: (from left to right) Hancock, Johnson, Plebeian Cannon Fodder, Doctor Blackadder, Jab Nurse
6th December 2022
Special 2022 Excessive Mortality Christmas Bumper Edition
Three years of personal, post-pandemic clinical testimony later. Time has not disproved my observations and experience. Still, the media, government and medicine turn a blind eye. Why? The below is a recent continuation of this telling of the horrifying truth. I feel like Blackadder.
2004 A baby from the past
A 13 month baby is seen in a combined neuro-ophthalmology clinic. She has perfect, limpid blue eyes. There is nothing wrong with them, yet, she is blinded suddenly overnight, a few days ago. From all the tests, it is presumed cortical blindness while we await further clarification. The parents are confused. Everyone is. She was developing well. There was nothing different the night they put her to bed, alone in a separate bedroom. I take a detailed history. The parents casually mention the day in question she had the MMR vaccine. Her mother had wanted to protect her baby, give her the best start in life. So had the nurse. It seems a good fit. But nobody above me seemed to bat an eyelid. I recorded the fact, making a deliberate show of doing so in front of the devastated parents. I never see the family again. I wonder about occipital lobe hypoxic damage after a febrile seizure caused by the vaccine. After all, apart from that, my medical programming states vaccines are safe and effective.
These days, a whole host of other vaccine-induced neurological causes will cross my mind. My standard advice to any parent after that was, if your child seems unwell do not put it to sleep in a separate room. If it has had a vaccine, give it an anti-pyretic before bedtime, fever or no fever. It seemed common sense. A few years later, I was chided by a nurse: we don’t do that anymore. Why? I did some research and the prevailing wisdom was if one suppresses inflammation unnecessarily, it could reduce vaccine efficacy. I was astonished. It seemed like it was throwing the baby out with the bathwater. Personally, I would now think twice about giving a child in my family any vaccine, and consider the research, risks and benefits carefully. Good nutrition, general healthcare and sanitation are more important. Multiple vaccines on the same day are increasingly routine for infants. No one really understands how they act or interact, nor the longterm harms of this blunderbuss approach.
2018 Dr No Vax
I meet my senior GP colleague and his 18 year old daughter. I am moved to remark to him, exceptionally, for someone who has spent a profession lifetime scrutinising live human specimens. Why does she look so radiant and healthy? He seems to have received the question before. ‘I know,’ he says in a matter-of-fact, clinical manner, ‘and no vaccines, only homeopathy’ (he is also a homeopathist). His own practice nurse reported him to the social services.
September 2019,Italy
A retrospective analysis of Italian serum samples reveals SARS-CoV-2 RNA and antibodies present two months before the Wuhan outbreak. Dr Jonathan Engler and his anonymous colleague performed an interesting analysis of this fact and the timing of the simultaneous mass deaths in different parts of Italy, April 2020 following Lockdown. They sensibly point out this does not fit a cause by spread of a respiratory viral infection, but does a cause of death by goverment policy. Democide. Eugyppius has ably summarised his key points.
18th October 2019, New York
Event 201, a praeternatural coronavirus pandemic simulation sponsored by the usual suspects.
4th January 2020
WHO Covid-19 pandemic declared. Attributed to a zoonotic coronavirus spread from a meat market November-December 2019, Wuhan.
11thMarch 2020 (circa) 10 Downing Street
Dame Dr June Raine, MHRA Chairwoman commented on a cabinet office meeting ‘about covid tests’ held with the Prime Minister, six days before the infamous Lockdown on 17th March 2020. She proudly admits her exchange with PM Johnson:
‘The question arose as, “Why a regulator was in the room?” Was a regulator going to be able to do anything about this? And our PM who seems to be able to notice things, shot a comment to me: “Well the MHRA will stop us killing people,” and for some reason, I was immediately able to respond, “No, the MHRA will help you keep people alive,” and that is the signal of the watchdog to the enabler.’
June Raine who has presided over the increasing dysfunction at the MHRA, much as Sir Simon Stevens did for the NHS, said this during her 5th March 2022, Somerville College talk about the transformation of the MHRA From a Watchdog to an Enabler during Covid. It sounds like a subliminal confessional.
The MHRA is here to stop State democide and keep people alive. Only a professional liar anxious to avoid conviction for murder can spontaneously split hairs like this. It may be Dr Raine need not wonder why she was immediately able to respond. In retrospect, it is clear from her words she as MHRA Chair abrogates from a duty of, and admits no intent of ‘stopping us (the government) killing people.’ One can read it as an internalised future vaccine alibi: I knew the MHRA’s negligence was killing people, but my focus, right from the very start was on saving people with safe and effective vaccines. In other words, it seems she is saying she is actively and openly in dereliction of a moral, official and professional ethical duty to weigh risk and benefit. June Raine’s transformation needs to be stopped and reversed.
MHRA Disclaimer: Medicines and Healthcare products Regulatory Agency Chair, Dr June Raine admits to categorically asserting to the PM that her MHRA ‘does not stop us killing people.’ Psychopaths have the tendency to lay their disclaimer at your feet at the very beginning. That way, it is overlooked.
Summer 2020
Lockdown is temporarily lifted for Eat Out to Help Out. I am sat on the grass munching a picnic by the roped boundary of a town cricket green. The sun is brilliant. The facing batsman is spectacularly out on the third ball. He has overestimated his abilities and incompetently slogged his bat into the hot summer air. In hindsight, it is reminiscent of Dr Fauci plays baseball. The locals burst into life cheering his demise. My myopia and vanity mean I do not know why. A few minutes later, our thin sector of spectators falls into a tense hush. Why, is not immediately apparent to me. A skilled voice with the intonation of a mean nose and small sinuses breaks the tension. “Hello”. It is a greeting mechanically reeled off from just inside the boundary two metres opposite me, from a man skilled in coldly managing hostility for his own benefit. I look up. TCP is within touching distance of Matt Hancock. Charity match, House of Lords team. The disgraceful, now ‘publicly disgraced’ unfaithful husband, and Ex-Health Secretary is enjoying his English summer recess after inaugurating the UK arm of a global, legislated killing and wealth redistribution program. How bad that actually is will become more apparent in the near future.
The first feeling is fury. I have scrutinised his role in my articles, and here he is, my muse. The crowd’s reaction is possibly more about his infidelity, but mine is because he was a key member of a joint enterprise which is causing continuous and current widespread human harm. I could have made a PR spectacle out of it. Spinned it. UnheroicNHSGP assaults Ex-Health Secretary. I could have verbally abused him, I could have overarmed my celery stick at him, tackled him to the ground, or far worse. The police would have classified it as an extremist terrorist attack, and TCP as insane. I would not be the first reasonable doctor to be legally-detained under a mental health act for questioning the covid narrative. That may well have been the learned and noble Dr. Thomas Binder, who was diagnosed with “Corona Insanity,” and then placed in a psychiatric unit. However, I am a pacifist healer. I do nothing, but sit in awe of how he could frolic with gay impunity within civil society.
February 2022
I hear on the grapevine the junior doctors in my local A&E revolt against their consultants’ request to get the third jab. The juniors refuse, reasonably asking why their seniors are not having theirs. It’s not actually that courageous or clever since they have had the first two, so ameliorating the threat of the sack in April 2022.
Late March 2022
Health secretary, Sajid Javid backs down from his jabs-for-jobs NHS ultimatum. He is soon to be gone and retired from parliament outright. I still have a job.
Summer 2022
A winter mortality in an English midsummer
There are an uncanny number, nay, an unprecedented number of electronic death notifications on my computer screen. It is not normal in my general practice. Once every working month or two, but not many a week, not a handful in half a day, not on multiple days in a week. There is rapid pause for sombre reflection. Excess deaths have been extraordinarily high in many countries, Not by covid, and not just the elderly. In fact, so bad in the UK the excess mortality rate is winter-like in midsummer. If this is what happens when the government tries to save us, it should stop trying. Further, there seems a correlative rise in mortality, immunosuppression and new escape variants of rogue coronavirus virus each time a new covid booster jab is rolled out. The government exploit the chicken or egg conundrum. Currently we are on jab 4. If you were classed as immunocompromised at the onset of the pandemic (arguably one is irreversibly immunocompromised in some way, after multiple covid jabs) one is on jab five, and counting. MHRA, VAERS and EudraVigilance data pointing to these being the most dangerous ‘vaccines’ ever, compared to all the rest combined in the last 30 years is old hat. So are abnormal rates of myocarditis, the worrying number of young people, pilots, athletes and indeed doctors collapsing and dying prematurely.
Surely, someone should be telling the patients being jabbed something about these concerns? Not at all. Why, they are Safe and Effective, always have been, always will be. Even if they are not. Vaccines are what they pretend to be. Patient safety has become a question of politics, philosophy and economics not science.
Even if nobody is telling them, surely there is an inescapable, uncomfortable truth that lies between government vaccine damage scheme and government ’safe and effective’ experimental gene therapy for them to see? Most are hypnotically blind to it. This paper is a reasonable summary of concerns, PDF here.
July 2022
Donbas UK Boy, 18
A mother of a local lad is worried. Her boy was in a good UK university. He has taken a sabbatical. He is graduating in Ukraine as a mercenary. He was depressed, and labelled with ADHD, hence he could not make the British army. He wished to make his estranged, ex-serviceman father proud. Make girlfriend believe he was brave. I carefully ask his mother if she is aware of accusations of Nazi undertones embedded in Ukraine nationalism. Oooooh, really? No, she is not. Nor I expect is he. He will fight and die amongst the Banderites, projecting his daddy issues on to The Donbas. We are all children of our generation’s state propaganda and educational indoctrination.
August 2022
Ukraine Mother with Daughter
The war has interrupted her cancer care. She has been fast-tracked by the Home Office Ukrainian refugee scheme. I have only just been able to understand what it is all about. There are language barriers. The young daughter introduces me to Star Trek technology: she silently hovers her smartphone in front of a Ukrainian medical report placed on my desk, and it miraculously becomes an on-screen semblance of intelligible medical English. Enough for me to refer mum to a NHS oncology department collapsed under the accumulative 20 year weight of government War on ‘Terror’, immigration and War on Covid policies, not to mention an aftermath of (non-covid) winter excess deaths in the summer. There is a striking correlation between autumn vaccine boosters and excess deaths in England. What will excessive winter excess deaths look like after the bivalent covid and flu jab Big Pharma Triple Wham in both arms?
The above three policies are inter-related. Two decades of EU-NATO wilfully destabilising the Middle East and Tony Blair’s transitional arrangements have brought a rapid surge of distressed, ill and non-English speaking refugees and immigrants into the NHS. Covid policy emptied and impoverished hotels, which then became combined covid and immigration concentration camps for these unfortunate souls. Caught in a devastated landscape of lockdown, they had to became rabid early adopters of covid jabs in their anxiety not to displease their new-found state. No doubt this phenomenon boosted UK jab statistics. Their coercion to the jab was greater than the average UK citizen’s. This rapid concentration of non-English speaking, culturally unassimilated, and psychologically distressed patients puts an incredible burden on an already broken and collapsing NHS, not to mention local community services. Imagine the effort and organisation it requires for a UN conference. All the technology and individual translators. This is the scale of the challenge for the United Nations’ NHS.
September 2022
8th September 2022 15:10 BST
The Queen is Dead. The British monarchy, is flying high off the back of 10 days of free global advertising and an extremely long queue apotheosised by the BBC. It is to be noted that King Charles III is a stalwart of homeopathy and organic farming. Does anyone who knows this believe he would actually take the WHO Jab times 5 or eat WEF GMO Soylent Green?
It is not just the rule legislators Johnson, Sunak, and Starmer, (the Ex PM, the current PM and the future PM) who break them, but those who preside over them. The future King William and family were snapped breaking the inconceivably diabolical ‘Rule of Six’. This is a royal family I could like if we were all treated the same. If only the family would realise the mental health sufferers they are fond of championing and joining are a product of the global system they helped create and maintain.
Autumn 2022
Just as autumnbegins to flutter itself in, I detect an elevated energy and mood in the corridor outside my consultation room. I had noticed there were more chairs crammed in the corridor alcoves than usual. Definitely no more than six inches apart. Optimism has betrayed me. It, I assumed, was a sign of a relaxation of The Arbitrariness of March 2020 – September 2022. But no. The NHS jamboree is just commencing. Rogue ‘Agency’ nurses dashing around in foreign medical garb. Intent, erect and in a mad rush.
I open my door to let out some of the various odours that inevitably accrue after a day of NHS consultations. Not least, that stench of my own habituated iatrophobia. Opening it admits in an inappropriate cheerful din in the form of a rat-a-tat-tat of regional accents.
Allergic? Had one before? There. Now get lost. Then follows a flurry of plebeian over-gratefulness, and a pitter patter of feet disappearing into an anaphylactic wasteland. I instantly recall last week’s autumn circular from our head nurse: It’s crazy season, again. Please let me know if you would like to take part in the vaccination.
30th September 2022, Land of the Free
Headline: California Governor Signs Bill to Punish Doctors for Providing Informed Consent Information Not Backed by Government & Big Pharma. Counter Headline, 4th November 2022: Physicians sue Governor.
October 2022
Genocidal Practice, Jabland, UK
Or should I say, democide? There is now a sort of self-selection occurring to those now on the fifth or sixth assortment of covid jabs. The coercion has abated, but the policy and messaging remains. The fearful, obedient and ignorant keep coming, but somehow even some of their children are being kept away from the killing queues.
Somebody whispers
There is another energised hum of fresh policy from the corridor. Foreign forces are mobilising again. Agency staff infiltrate the building and mingle with the regulars. Some unknown, mercenary male nurse apprehends me as he attempts to requisition my clinic room. He dissembles and shakes a social front from his wrought face, “Oh, hello. Are you vaccinating?”
I stare at the baggy man, who offers nothing else, and offer him a studied careful, “No,” followed by a pause heavily impregnated with, of course I’m f*****g not, I’m a proper doctor. His body shimmies, he mechanically turns and disappears. A more distant, rising bleat of Joe Public is building in the waiting room. From the corridor, there is a professional lull.
Then, our head nurse is heard to whisper …
“Shall we wear masks?”
It was a stunning pantomime confession. Not that I can be stunned anymore. Her Freudian whisper acknowledged all knew it was an inconsistent scam. It did not shame her, she merely wanted to know how deep should they fake it.
Cleanliness is next to Godliness
Crazy season was crazier this year. Six antigens: quadrivalent flu, and the unpredictable bivalent covid genetic pre-antigens. Plus patented God knows what. God reminded of me of my American cousin, the religiously-inclined Dr Ashok Jha, White House COVID Response Director. He says to the public with a barely suppressed smirk:
“Get your Covid shot. Get your flu shot. That’s why God gave you two arms…”
On a normal day these were equal grounds for blasphemy and dismissal from the profession. But we live in a time where mores, ethics and normative principles have been obliterated. There are no religions, no professions, no norms. There is no gender, no childhood, no rights. What remains are only centrally controlled, evil but ridiculous State edicts and diktats.
“Get your Covid shot. Get your flu shot. That’s why God gave you two arms…” Dr. Ashish K. Jha, White House COVID Response Director
Were they going to do that in NHS, England, too?
Finland is not recommending the bivalent. I resolve to enquire on my hurried exit away from my genocidal colleagues. Faux-masked head nurse is standing with hi-vis vest and clipboard. There is an obedient queue of hypnotised, silent fodder with no social distancing. Evidently the imminent jabs provided seamless protection from their last. The queue trifurcates into three consultation rooms with open doors. Negotiating the corridor is like being captured in a hypodermic pinball machine.
Is it covid or flu, love? Both. Ok, have you survived them before? Yes (not true: not at the same time and not these particular concoctions). Ok, love in you go. ‘Love’ is in and out through the staff side exit in seconds. I stop in the corridor and ask the head nurse, “Aren’t they waiting before leaving?” The answer is no. She looks at me, in a crazed fluster. I am reminded of my response to her recent email: do you want the flu and covid? My terse reply: I am making my own arrangements. Time to go, before I am found out.
Dr Either Or
From a distance, my GP colleague gives his version of informed consent and bodily autonomy, ‘Do you want both in one arm or one in each? Both are fine by me.’ It should not be but it is. So the devout Dr Jha was wrong. God did not presciently give humans two arms for this specific world event.
Mrs Vaccine Allergy
In the jab frenzy, one lady patient does audibly declare some kind of covid vaccine ‘allergy’, but breathlessly appends a hurried apology, ‘but not to the flu (vaccine).’ It sounds like she had rehearsed what she should say in her mind before entering Jab Central Station. Clemency was given. She must have left feeling like a dead man walking leaving the gallows.
I wonder about her later in the end-of-day fugue that accompanies the job and a tired, old brain. What did she mean, exactly? Was it patient code? Did it mean, I’m reaching a compromise, to please you. I’ll take that unproven, speculative but relatively safe flu stuff, but not your botched bivalent blockbuster at triple warp-speed, thank you. Not after the serial monovalent massacres.
Maybe that was my wishful thinking. But there is an even more serious point. Where are the informed consent and the formulation of a patient-centric decision arrived at after a consultation between the patient and a trusted doctor nominated by said patient? There aren’t any.
I think of a different, recent, even more satanic time, when exemptions were by politburo and virtually impossible. What if the patient had been responding to an offer of covid jabs 1 and 2? Declaring a previous vaccine allergy was next to useless. One had to have nearly died of covid 1 to avoid 2. Number 1 was nearly unavoidable. Don’t believe me? Memories are short.
What suppressed carnage would the bivalent covid jabs wreak? Would nurses continue to jollily administer them, after all we know? There remains a large, malleable cohort of dutiful, trusting, and terrified patients. I struggle to concentrate on my work, but there are odours to exorcise. The door remains open.
NHS SMS SOS
NHS SMS flu and bivalent covid jab invitations are being cascaded to those aged 5 years and over. In spite of the contrary science. I am beginning to see the first wave of patients telling me they have fallen ill days after a combined double-jab, aka the Triple Wham. Chest infections and melaena are amongst my first compartmentalised, clinical anecdotes of side effects, never to see the real light of day because of the deliberate policy to suppress adverse events and promote a safe and effective lie.
The whole matter stank like a heap of steaming shit from the very beginning, yet all these professional medical and nursing numbskulls complied. Even many of those who now admirably crusade against the covid narrative.
‘Having Covid’
I, an unvaccinated GP, within earshot of this relentless conveyor-belt, should not be here. I should have been dismissed from English medical practice, 1st April 2022. Some of my patients still tut-tut to me about the non GMOs. The irony is of course massive, not least because some of the most rigid are those chesty ones who acquired bad bacterial respiratory illnesses without, or with likely coincidental or false covid positives. The type of illnesses which happened before and after 2020, but doctors no longer acknowledge. Many patients prefer to re-classify these as ‘having covid’ for sheer dramatic effect. They seem deflated when they tell me they ‘had covid’ and I remain unimpressed. I do not treat tests, I treat patients. This, they find very confusing.
Mrs Empyema, 57
One pleasant patient in this faux-covid bracket listened to the application of my strict diagnostic logic in her case. She had spent 6 weeks on intravenous antibiotics for an empyema, and double pneumonitis. I rapidly précised the late 2020 hospital notes. One could hear the enlightened, bunkered radiologist screaming off the report page, in full knowledge that he would be ignored by everyone: THIS APPEARANCE DOES NOT NECESSARILY IMPLY COVID INFECTION.
She listens to my opinion, impressed, until I point out the [pseudo-]vaccines were neither preventing transmission nor infection. One can visualise her potentiometer dropping several ohms to extremely patronising, her tone and pace lowering, her cadence distorting and she emits in a slow motion, ‘Oh … come … o—n.’ I could have, too. By countering with the legendary brown notes, ‘I’m unvaccinated.’ But, one knows how clinical odours must be regulated.
‘Oh … come … o—n.’
Tuesday 11th October 2022, European Parliament
Janine Small, president of international markets at Pfizer is asked by Dutch MEP Robert Roos whether the Pfizer vaccine had been tested on stopping transmission of the virus before it entered the market. She admitted it had not. The vaccine and vaccine passport are scams. The state lie was gargantuan, the media reaction is negligible.
Hallowe’en in the first week of November 2022. The descent of winter darkness is reminiscent of 5 months ago. Ping, ping and ping goes the computer screen. Three death notifications in one working morning in a small general practice is unprecedented. I nonchalantly remark on it to test the water in reception. ‘Oh, there was a fourth just now,’ breaths the young receptionist, anxiously. I looked at their senior, and quip, ‘Anything to do with the double (I make cartoon jab movements to both deltoids)? Feels like eugenics.’ Their captured eyes betray closet agreement. They know and suspect the same. I defuse the tension as it heightens by catching the concerned eyes of a third, “Cheaper housing.” There is a confused grimace, in response. She has scruples.
I check two of the four dead, both retired, previously well and perfect subjects for the flu and bivalent covid jabs. One dead four weeks and the other dead 3 days after the Triple Wham. It does not bode well.
The mask police are back with diminished authority
A return after the Hallowe’en weekend reveals the practice has arbitrarily re-imposed a mask mandate via SMS upon patients. The covid propaganda machine is revving up for winter. It is nearly three years after the pandemic and some of them are on 6 jabs. Still they comply and tremble. How long can this go on? It is a product of a financial elite imposing a belief system on the masses via a state apparatus.
Like a mother to a 7 year old snotty-nosed school boy, a young receptionist tut-tuts me in the corridor, admonishing with a “Where’s your hankie?”. ‘How can I tell the patients to wear a mask if you are not?’ I ignore her with an anarchic raised brow and a purse in my lips, peering over her masked head and call in the next poor victim of NHS communism.
So here it is, a conspiracy policed by young medical receptionists. It is my fault for not reinforcing the Lie. Naughty, ethical doctor. She is a projecting purveyor of murderous bullshit, of patently phoney propaganda. That the UKHSA has never countenanced anything but a safe and effective vaccine says it all.
Quite a lot of the grey brigade in the waiting room sit quivering, recalcitrant, unmasked and surly-faced. I feel them. They cannot take it anymore. It is the first time they have ever rebelled against authority. When invited by me in the safety of my consultation room, with varying degrees of dissemblance and thanks, all rip them off as if they were used toe-rags.
Guide Dog
There is a guide dog in the waiting room, it is not masked. It is not facetious to observe this. I have not forgotten. If your infant granddaughter were not enough to satiate your endless covid phobia, the propaganda attempted to turn man’s best friend into a cold, killing assassin, not to mention other pets.
Black November 2022
The NHS zeitgeist is evermore ‘precarious’ and ‘hopeless’. Patients passively accept a NHS ‘no-care’ policy. This month, the waiting rooms and the corridors are palpably colder than usual. But the clinic rooms are still mercifully warm. Is this more subliminal propaganda? Pensioners sit shivering in the NHS waiting room. It is an unwelcome and untimely full circle for them. At its birth, the NHS used to do something similar when they were children, to treat TB. It befits the end-of-times ambience which supranational and national state entities have curated with cynical skill and intent.
The silent, cautious eyes of schoolchildren
Children have also grown weary of state assault and a parental instruction: do not let them put anything in to you. Well-meaning, brainwashed, socialised school and social workers are denying parents liberty on many levels and conniving with biological assaults on little children. One may think they are lost in a make-believe world of smartphone passivity. I do not believe they are. They are watching and listening, when their time comes, this generation will not forget and will react with unpredictable social ferocity long after their abusers are decrepit and gone.
6 year old anti-vaxxer, pro-healther
A message pops up on the screen. Covid gene therapy virtue signalling. Well done, Everyone! Yesterday evening, a little girl who was, rather sanely, absolutely terrified of the unpredictable and unproven bivalent covid-19 jab was successfully persuaded to have it. Wellbeing Success! Or is it legalised, ritual child abuse, assault and attempted murder? Really well done to everyone involved!
There is no reason for a child to have this unquantified toxin. It is a spine tingling moment from a spineless movement. One not open to being open. Are these folk nuts? No. We are. In Ontario, we are to be counselled and medicated psychiatrically. Yet, in fascist Ontario, there is some light. An apolitical judge with nuance, science and sanity has found a mother can save her children from the covid jabs. The judgment deserves more attention.
Glamorous corporations like Balenciaga are promoting child abuse in astonishingly open ways. Like covid abuse it is an open secret which hardly anyone sees, questions or protests. Children have an especially unlikely and unpleasant place in covid, too. Why is there an unrelenting drive and public discourse by media, governments and Pharma (not least by Pfizer chief, Albert Bourla) to serially reverse-pimp an unnecessary, dangerous experimental gene therapy into the arms of our children? We know it provides a liability shield in the US, but that is no reason, and not enough globally. No one cancels either of them.
Deranged College of Physicians and Surgeons of Ontario recommends psychotherapy and psychiatric medication for humans making reasonable personal health choices.‘Pedo-chic’: fashion world aestheticising child abuse.
CrewcutGirl, 12
This cool kid has a healthy fear of doctors. As an aside, her mother asks, ‘Do you deal with the covid boosters?’ I cannot workout if it is subliminal virtue signalling or whether mother may have been carefully selected me as someone she could trust to ask for considered advice. I give it. Daughter is pleading with her mother to agree with me. Maybe they had been contesting the point for sometime. Perhaps, Crewcut had read my counter-propaganda. Maybe the mother wanted a person in medical authority to say it was ok to say no. Crewcut fist-pumps the air in relief at the acceptance of my independent opinion. My conduct is what the type of totalitarian medical legislation proposed in California and Queensland is designed to stop. They are desperate to force, coerce and dupe everybody into an unnecessary dangerous biological intervention.
The Student Nurse, 23
What is it that is taught in medical schools and nursing schools throughout the globe this year? Have university revised the medical curriculum to follow the Syllabus according to Tedros, Gates and Devi Sridhar? Is it the scientific lie perpetrated in the last three years or the eternal truth of critical thinking, ethics and evidence that prevails in our captured institutions?
One young patient provided a taste of an answer. I lament to her that any current student or junior of nursing and medicine in a hospital had a bad start. Malpractice, fraudulent covid death certification, uncritical and unethical thinking has been their constant diet. She nods in ready agreement like someone who has not tasted water for years. Professional behaviour had ‘gone crazy’ in her hospital. Innocence is refreshing. Is anyone challenging their lecturers, matrons or consultants on the gaping gap between nursing theory and covid practice? No.
A problem for the layperson patient is trust in health professionals is so ingrained one would assume against better instinct that if the government were wrong in its medical advice, any doctor or nurse would instinctively curtail that risk in the patient’s best interest. That is exactly what is not happening. Many health carers have behaved like laypersons and worse. Ignorantly, or in pure obedience to stakeholder capitalism (fascism). They are failing their patients cognitively, ethically, and scientifically.
Ms Arthritic Baldy, 52. Frank information = Misinformation
A brave outlier patient with spontaneous, and worsening alopecia areata asks me whether the covid jabs could cause it. It can. Strangely, a few weeks earlier, her joints swelled up transiently, too, I only just noticed in the frenzy of a second 10 minute consultation (all basic and rheumatology screen blood tests negative, no personal or family history of rheumatological issues). She only asks because her hairdresser has seen a covid-related spate of baldness. I decide to repay her frankness in kind, after all, we UK doctors have a duty of candour. Even if the UK government, Big Tech, Ofcom and the GMC arbitrarily and selectively help suppress it as ‘misinformation’. She has had a dolly-mixture of jab brands, and regardless of her concern has returned recently and got the fifth. These could well be the cause of both her alopecia and arthritis.
I explain that I will be frank, in spite of being de facto censored by state threats, constrained by propaganda and may in the future be legally prevented from giving my independent, bespoke professional opinion. This, reassuringly, shocks her. MHRA stats? No idea. General jab concerns? Only what the hairdresser said. Clots? Oh yes, think I heard something about that somewhere. It is a remarkable cover-up in plain sight.
Three Sexagenarian Siblings, 60s
All in their 60s. Two hospitalised, one dead. Little brother collapsed before his shift with a massive myocardial infarction 2 months after last winter’s jab 3. Three resuscitations, three coronary stents, and 6 months later he is finally dead. One sister, also after jab 3 is simultaneously hospitalised by a brain clot in the same hospital as the brother. The other sister is now feeling terribly unwell after jab 4. They cannot see any connection. Will the surviving sisters be properly dead after number 5 + flu? We shall soon see. For those that can, it is like living in hell.
Another patient tells me she stopped at two jabs because too many people were dying soon after the flu/covid jab combo last winter. These are the deeper, incontrovertible statistics that cannot lie, cannot be proven and will not be acknowledged. They lie deep-rooted in family and community consciences. The statistics of the immediate and longterm damages of the jabs to the general population will be damning, should they ever be allowed to see the light of a non-politicised, impartial analysis.
Why are coroners not calling it out? It is their professional duty, regardless of definitions to call a spade a spade, a suspicious death a suspicious death. Some doctors, nurses and funeral directors have, but not many coroners. They, too, must be witnessing the unusual death activity. All one has to do is look at the relationship of jabs to deaths to confirm the concern. Nobody in office is. And so the killing will continue.
Mr Sepsis (divorced), 75
He is a lucky man. His ex-wife is literally nursing him back to health, wiping his balls and bum clean whilst he remains incapacitated. We joke, how does he do it? What is the secret to his endless charm? He had been hospitalised with a severe sepsis. They are both intelligent and well-informed. We get on. As they leave, she turns, sensing an opportunity. In that innocuous, self-effacing tone that only the upper classes can feign, ‘Oh, doctor, should he have the flu and covid, yet?’ I step back and measure them more. ‘Oh, I wouldn’t do that just yet. Why complicate matters when you are only just recovering?’ Her body in toto speaks of relief. She has found an excuse with which to fend of societal opprobrium, to protect her daughter’s father. I venture further, ‘Besides, many don’t seem to be doing too well after getting both in quick succession.’ There is a tacit agreement from them. They know this. I go further, ‘At least space them out, or if you wish, don’t bother at all. Do what you want. There isn’t even a pandemic.’ They leave smiling, relieved of state shackles.
Mrs Chestnut, 83
In response to a ‘feel free to take off your mask in my haven of science and logic’, this 83 year old, with impossibly chestnut hair delivers a possible conspiracy theory! ‘Doctor, do you know what I think?’ There is no pause, I have already invited myself to her thesis. ‘This virus is created in a lab to kill old people.’ Not bad, it fits. I accept the gauntlet. ‘What do you think of 5 jabs in 22 months?’ Silence. ‘Do you know the jabs were sold on an impossible lie?’ Silence. ‘Transmission and infection not stopped and possibly augmented?’ Silence. It seems I had her at mask but not vaccine. I stop and sort out her neck. It does not seem right to discuss the vaccine risks with a card-carrying convert on a fistful of jabs. For her, it is the creator of the virus who is the geronticidal maniac, Not the democidal genius behind endless genetic modulation. She has not considered it is the same behind both.
Edna Amnesiac and Peter Coincidence, 86 & 87
The next patient case is Edna. It is complex, not least for the haphazard hospital discharge letter written in broken logic and non-syntactical English. This is the smallest of its issues. It is riddled with factual errors and lacks a diagnosis or a conclusion. In the rush to turnout a patient, it spills out some tests done and some changes to the medication. It is left to me to forensically remake the letter. I know ten minutes are not enough as I canter over to call them in. Saving seconds means everything in this job. Edna is joined by her supportive husband, Peter. It takes nearly a minute to stand each other up and another two minutes to walk in without either of them tumbling into the magnolia-painted walls. I am distressed by their story.
She has been out a week, has no idea what went wrong. No idea she has missed a first appointment to check her kidneys post-discharge, and no idea her second is soon, to ensure her CRP has fallen from a hospital measurement of 172. CRP is a non-specific serum marker of acute inflammation. You don’t see them this high normally, even in ill, ill patients. Less than 5 is normal, and in general practice, anything over 50 might make one sit very upright. In a nutshell, she collapsed at home, hypotensive and semi-conscious. CT head NAD, presumed sepsis, ?cause. As soon as it can get rid of her the hospital does.
What exactly happened to cause her decline and hospital admission, I ask her more orientated husband? Peter sounds weak, too. ‘I don’t know.’ Why ever not, sir? I am irked out of concern for a consultation collapsing into directionless chaos…
‘Because I went into hospital, two days before Edna.’ This kind of unlikely coincidence is more often these days. The gauge of my internal jab-o-meter convulses abruptly.
I peer at Edna’s notes. She had the triple whammy – bivalent covid and flu jabs – 5 days before she became critically ill. She still looks awful and can still barely walk. The hospital had not even mentioned this crucial clinical event which had nearly killed her, and still might. Just like the baby from 2004, a multiple jab followed by a catastrophic biological inflammatory event. And no recognition of this possibility from the medical or nursing professions.
Peter continues, ‘Last year she also had both together and could not get out of bed for a week.’ I ask them how they feel about the fact the jabs don’t do what they say on the tin, how they nearly killed her and how she is on her fifth: ‘Well, we’re just doing what we’re told.’ How do they feel about future jabs: ‘Well I don’t really think we want them.’ Will they cave in again? Most likely. Will they survive it? Spin the wheel.
I interrogate Peter’s notes. He had the double jab 4 days before his hospitalisation. When our nurse visited him at home to triple wham him, he didn’t jab the wife. Peter panicked, he called the nurse back to his home to do his missus. That nurse is the Agency one who in October tried to requisition my room. It should not go unappreciated that their are thousands of Ednas and Peters globally. Some of them survive, some have a reduced life expectancy, some die quickly, some surreptitiously, but never will a jab delivered by a government agent be the culprit.
Nurse Agent 007
Our 007 of retired Nurses is still grifting a few quid to top up his NHS pension, fancy new car, Walther PPK syringe and silencer, Licensed to Kill. He enters and leaves through peoples’ trusted front doors wreaking domestic and community chaos as if nothing ever happened. Likely he has no idea. Only I see his aftermath.
He has either assumed I am one of his cult, or one of the covid underclass. On two occasions he has chased my buttocks with an imaginary jab-action shotgun down the surgery corridor in a slapstick Carry on Nurse capering style. The first time, I called his bluff and bent over double to present my rump in mockery. The second time he tried it on, his having not sensed the pathos of my first bluff, sent shivers up my spine. He was entirely impervious to the risk and nuance of his being an accessory to the greatest medical scandal ever. Nurse 007 is not very bright. He strikes me as the cannon fodder of frontline warfare, a blunt instrument positioned dangerously with an automatic weapon.
Mr & Mrs Octogenarian Neighbours
My dear neighbours Claude and Iris are conspiracy realists. After jabs 1 & 2, 2021 Iris was hospitalised with a lower gastrointestinal bleed, and Claude was left at home to descend into an unanchored abyss. She survived and lived to book them in for 3 and 4. They looked at me as if I had gone mad when I entreated them to not be so cavalier. This winter it is different. Iris is a renaissance woman. She has been to line dancing and heard that they are falling ill in droves with the triple whammy. Neither she or her husband are having either: ‘Five jabs and still testing healthily covid positive? Why it’s rid-ic-u-lous!’
Mary, Mary Quite Contrary, 94
Sherefused the 4th jab, she entreats me in a weak voice over the phone, ‘Please tell them to stop sending me reminders for the fifth, doctor – it is like torture.’ I know the feeling. It is worse than those never-ending TV licence letters threatening fines and surveillance. I’d rather watch the BBC than be jabbed. Not that I watch its propaganda or have a licence. ‘Of course, Mrs Contrary,’ I rattle off a task to reception as we talk: STOP INVITING PATIENT FOR COVID JABS, IT IS DISTRESSING HER.
She continues, ‘My friend had to have them to keep her job at the care home. Ohh, doctor, I’ve never seen such terrible times.’ I think about that statement. Here is a lady born in 1927, child of the fall-out of WW1, a survivor of WW2 and an existential Nazi threat. WW3, Globalist Elites v Humanity has been far worse for her.
Grandma TCP, 95, A voice from the grave
As some of you will have read here, in early 2021 Grandma died aged 95, no medications, and all marbles, sphincters and limbs intact. It was a rapid demise over 5 days from heart failure. Normally, a cause for celebration of a healthy, long life. The NHS were determined to sully it. It was the usual ploy, put her on a covid ward to die, hope she tested positive for covid, and even if she did not, list covid as a cause of death, as if death on a covid ward was reasonable belief enough. Doctors are required to certify causes of death “to the best of their knowledge and belief”. She even tested negative on the ward, but that did not stop them putting her there, nor the junior doctor writing covid as a cause of death. We challenged it as the ink was still drying. A rapid scurry and revision corrected the insult to a simple dead woman. This wilful, semi-conscious NHS forgery has been happening on an industrial scale. Falsifying death certificates is a criminal offence.
It gets worse, sadly. One and a half years later. There is a voice from the grave. An old friend calls after a long time. Grandma was actually hospitalised two days after jab 1, and dead 5 days later. We know because she called her old friend, upset. The NHS and next-of-kin held her down and got her done. Another mortal snatch and grab. She was coerced into it by them. Sudden cardiac death is a real, established concern after covid jabbing. She will not even be recorded as a vaccine death, since the crooks define vaccine death impossibly. She was against medication, even a vitamin.
The irony of the NHS death certificate falsifications, definition doublespeak and statistical fraud is not lost in my personal distress. If I were wishing to legally try get rid of an elderly relative, I would book a simultaneous bivalent and flu jab and scarper, hoping for the very worst. For good measure, just add a shingles and a pneumovax, too if they qualify. A GP practice will quickly arrange a domiciliary visit. Such are the pecuniary gains. Where doctor home visits are in short supply, our practice is only too glad to send out a cheap nurse agent for a pharmaceutical accumulator.
These are the most vulnerable to the Big Lies of Covid: the most medically vulnerable. They are the infirm, unwell, and cognitively-impaired sitting alone in cold homes and lying exposed in nursing homes. No relatives to shield them, no accessible, alternative internet information to inform them. They are medical fodder, and lambs to the state slaughter.
‘What can we do?’ say slayers and slain alike, ‘We’re just doing what we we’re told.’
14th November 2022, London
Dr Aseem Malhotra, mainstream popular cardiologists calls for the Moderna and the Pfizer jabs to be withdrawn in his talk, ‘Has Big Pharma Hijacked Evidence-Based Medicine?’ It is sensational and damning content for the uninitiated masses. It does not make the mainstream news. Their interest is in investors, not human safety. The cover up is only possible because the inequality of arms outweighs the pristine truth. Dr Malhotra’s two covid jab research papers can be accessed here and here.
Dr Malhotra drops truth bombs. Media: Silent
Winter 2022
Killing Fields
Total Practice deaths: 8 in October, 20 in November. None of them of, with or by ‘covid’.
Mr Slow Killing, 81
Interred indefinitely in a care home, nowhere to run, nowhere to hide. Chest infection, 14 days post triple whammy, never recovered. Dead 6 weeks post triple whammy. Placed on to an end of life protocol. Surely the jabs were the way to prevent this type of respiratory disease death? No one makes a link. The statistics if ever they see the light of critical day will not lie.
Mrs Frozen to Death, 83
The final death in November is an 83 year old female, recently given oral antibiotics for a mild chest infection more likely acquired courtesy of deliberate, manufactured energy poverty policy. Found hypothermic on living room floor, no heating on in the house. Dead in hospital 24 hours later. Her cold corpse an effigy to the determination of EU-NATO to crush a post-USSR, multipolar and diverse world at the expense of the wider, world population.
I compare these monthly death rates in a 10,000 patient practice to the 5 covid deaths in nine months by September 2020 (all elderly and with co-morbidities) in an accumulated practice population of 16,000. This during the peak of the pandemic hypochondriasis and hysteria. The US, Germany, and Australia statistics are showing similar concerns.
What will December and January bring? This is the UK, winter 2022. More doctors, more money, even more morbidity and mortality, and a deliberate policy-led, ritual lynching of us and the NHS on behalf of the corporates who eye the private health pie an NHS death will bake. This is why the NHS can no longer cope.
ONS week 46 data. Since 1st April 2022, 30 of 34 weeks have produced excess deaths in England & Wales. Average excess deaths over this period have been 1,164 per week. The total excess deaths for the entire 34 weeks equals 39,591. By the end of the year, this could approach 60,000 excess deaths. This would challenge the 2020 corrupted statistical covid pandemic deaths. Silence from Media and Government. No one in government panicking, locking down covid vaccination centres and building Nightingale hospitals and vaccine damage centres for these dead. If this is the excess mortality, the excess morbidity may be orders greater.
The First week of December sees the temperature in the consultation rooms fall to barely comfortable. The weekend sees the heat completely switched off. Mondays are intolerably cold, now. My straightforward ultrasound, CT scan and MRI requests are regularly being declined by anonymous bureaucrats who have never seen nor examined my patients. This is new. If I am to obtain scans, I now must seek permission from a hospital specialist. It is another unnecessary inefficiency and ill-health initiative inserted into the collapsing NHS algorithm. An MRI scan now takes 7-8 months and rising to come to fruition. Appointments with hospital specialists are almost a thing of the past. If one is obtained, it is commonly very delayed and by telephone. A referral by a GP to a hospital colleague has become superseded by a desperate plea for hands-off written advice, in recognition of the impossibility of a timely referral. By its pretence to offer appropriate care, NHS policy and conscious mismanagement is killing its patients.
Mr Extremely Mesmerised
Another cult message on the surgery computer system, Mr Extremely Mesmerised has messaged us on last night’s out-of-hours jab-rave. He writes, ‘Wow! So efficient. I barely sat down. It ran like a well-oiled machine.’ If only the same could be said for normal healthcare in the remaining 99.9% of the NHS. The last time medical staff worked with such clinical efficiency may have been Nazi Germany.
1st December 2022
Dr Chris Whitty, Government Stooge
His job today is Limited Hangout. Lockdown was Democide. He sounds surprised. Why? We all knew it was. Reading between the lines his headline should read: People, prepare to continue to die more. What he does not yet acknowledge is his jabs killed, are killing and will continue to kill. For the time being, by this incomplete admission they are preferring pharmaceutical share value over a complete, open rubber-stamping of totalitarianism. It is a small victory of sorts.
Whitty ignores the very real contribution to escalating cardiac disease and death his continuing jab recommendation is making. Seemingly oblivious, health charities such as the BHF see, hear and speak no jab risk. Why would they risk their state-corporate funding? Instead, Whitty focuses on cancer deaths caused by missed diagnoses, but not on cancer-causing covid jabs. This is telling.
Covid Jabs Causing Cancer
Whitty should be aware of this serious concern. Professor Angus Dalgleish, oncologist, Dr. Michel Goldman, immunologist and any sentient generalist like me is.
B-Cell cancers
Professor Dalgleish outlines serious, cogent concerns about covid jabs in this concise letter to the BMJ, watch him speak with Dr Tess Lawrie, here and below.
Professor Angus Dalgleish & Dr Tess Lawrie. (34:42 – 35:52) re. jab immunosuppression promoting cancer, “What we are seeing now is people are ok until they have the booster … the regulators have a duty to see is this really true … It’s not going to show up in death figures for several months, by which time it could be a catastrophe.” I agree. It already is.
T-Cell cancers
Brothers, Drs Michel and Serge Goldman report an extraordinary but not exceptional case, here. It is a very concerning: a T-cell lymphoma developed 5 month post Pfizer 1&2. Rapid Progression after jab 3. The first medical author is the radiologist brother of the corresponding author/immunologist/patient. Booster jab 3 was given in an erroneous attempt to protect this ‘immunosuppressed’ patient prior to chemotherapy. That the immunosuppressant jab seems likely to have caused and progressed the lymphoma is very ironic. Spoiler alert – the patient still feels jabs are worth it; writing this may be the price paid to achieve publication.
Dr Michel Goldman’s post covid jab, and post booster lymphoma-ridden body, see report, here
2nd December 2022
Midazolam Matt
Matt Hancock, Democidal Maniac, MP has successfully transitioned to Democratically Elected Celebrity. This is more careful perception management. He is an immoral and unethical lead actor in a criminal joint enterprise. Boris Johnson’s father says Hancock should be forgiven. Evidently, the globalists want their best Dr. Mengele back, rehabilitated by hook or crook. Back with more skin in the eugenics game. Why wasn’t he made to take the midazolam challenge in the jungle? His participation was key in a horrific, wholehearted, ritualised looting, torture and killing of our people.
Hancock has determined on his return he will marshal a brotherhood of dyslexics upon parliament as an artful distraction. It is as if he is mentally writing his own sick-note. Why won’t he join forces with Sir Christopher Chope and fight for the jab-damaged and dead? That is where his expertise lies, and that is where a champion is desperately needed.
Hancock’s dyslexic Diary of a Political Sociopath, true to his narcissistic personality admits no fault, no responsibility, no remorse. He defends from behind the unreasonable hyperbole of his own faux covid propaganda, hiding behind a quote from Chris Whitty who ‘warned officials 820,000 people in UK could die from COVID’. It is not true. But what could come true is more will die from his government’s covid policies made on his watch. He points a crooked finger at Ex-NHS boss, Simon Stevens. They are finally turning on each other.
Hancock omits all the important facts. He was aware of these. Many doctors wrote to him and the government to raise concerns, including the UKFMA and me. These kinds of speculative, propagandist estimates were unreasonable, even at the time. It has been ably demonstrated none of his covid measures had a hope of being helpful. Toxic policy, toxic jabs, toxic personality. No doubt when all excuses founder, he will take to blaming dyslexia for his failures and misconduct.
“Authorisation has today been granted for a new presentation of the Pfizer/BioNTech COVID-19 vaccine (Comirnaty) for use in infants and children aged 6 months to 4 years.
The Medicines and Healthcare products Regulatory Agency (MHRA) has authorised the vaccine in this new age group after it has been found to meet the UK regulator’s standards of safety, quality and effectiveness, with no new safety concerns identified. This decision has been endorsed by the Commission on Human Medicines, after a careful review of the evidence.
This presentation is specially designed for this new age group and given at a lower dose compared to that used in individuals aged 5 to 11 years (3 micrograms compared with 10 micrograms). It is given as three injections in the upper arm, with the first two doses given 3 weeks apart, followed by a third dose given at least 8 weeks after the second dose.
In reaching their decision, the MHRA’s experts carefully reviewed data from an ongoing clinical trial involving 4,526 participants. The common, expected side effects (reactogenicity) were in-keeping with what can be anticipated from a vaccine in this age group.
It will be for the Joint Committee on Vaccination and Immunisation (JCVI) to determine if the vaccine will be recommended for use in this age group as part of the UK’s COVID-19 vaccination programme.”
This in spite of all the known dire jab risks, jab ineffectiveness, no extant pandemic, no risk to this group, outdated variant-specific formulations, and despite a study published in JAMA of 7,806 children aged five or younger showing 1 in 500 hospitalised with jab adverse-effects, and one in 200 had symptoms ongoing for weeks or months afterwards. Surely the risks far outweigh benefit or need? Read the combined response to the JCVI of the excellent, evidenced and ethical CCVAC (Children’s Covid Vaccines Advisory Council) and HART (Health Advisory & Recovery Team) Group.
Why does anyone trust Dame Dr June Raine? She believes her MHRA duty does not include preventing the government killing people. She believes her Gates-funded MHRA is transformed from Government Watchdog to 86% Pharma-funded Pharmaceutical Enabler.
8th December 2022
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org
Sincerest thanks to Bob Moran and The Democracy Fund for Bob’s cartoons.
The Covid Physician is (still) an unheroic NHS doctor. This article is a personal view and does not necessarily represent the views of the NHS. Patient details have been anonymised.
Drs Fauci and Whitty. Their covid policies have, arguably, contributed to the greatest consequential harm to world health and mortality in history. The full sequelae have yet to be realised and are ongoing. Their policy conduct during covid was so reckless and grossly negligent it may be criminal, in my opinion. Whitty was knighted in 2022 ‘for services to public health’.
10th August 2022, Seattle Mariners’ stadium. There was something rather emblematic about the most powerful and worst doctor on the planet getting it so publicly wrong. It was as if he were in real danger of throwing the baseball in a diametrically opposite way to his purported intent.
Fauci was bathed in baseball fan cheers at the start of his pandemic roadshow. Feelings have since changed. The sheer audacity of him prancing on to the pitch like an elfin Peter Pan into a coliseum of rednecks at the end of a trail of medicalised slaughter is a definition of pathological denial. If only he could soak up the propagandised adulation of the masses once more before announcing his retirement, it may in his mind prove he is always right. That he and Gallo did deliver a vaccine against AIDS within two years rather than actually fail to for nearly forty.
It should have been his natural safe-space. A Washington home team playing the New York Yankees. But it was nothing of the sort. They booed him as he risked propelling the baseball into his face. No matter, he is infallible. He raised in hands like a gladiator, perhaps, more surprised his shoulder did not dislocate.
So Fauci is retiring, but not, he says, in the classical sense. As if expiring young people wasn’t enough, in retirement he wishes to inspire them. He cannot take their parents’ hint. They, the world over, have already let him know what they think of his final medical act by finally saying, no jab for little Johnny. What would he teach those children? Gain of function, how to be a sociopath, how to harm everyone and nearly get away with it?
The same goes for Whitty. This doctor signed the medical prescription for the Lockdown and the jabs. The, then, new Chancellor, Rishi Sunak says he and others dissented, but the executive was editing the SAGE minutes. Rather than blow the whistle, he became the most profligate accessory to the multiplicity of crimes misconducted in public office. He bank-rolled the whole sham, inducing the country to self-immolate in an orgy of fear, nasal-swabbing and experimental gene therapy.
In 2021, they appointed the AZ jab women Dame, and more importantly, Barbie Shero. They gave her a standing ovation at Wimbledon 2021 just as the clots commenced congealing countrywide, and just before they were locking up Novak ‘Novax’ Djokovic in an Australian clink.
Pharmaceutical-grade child propaganda. Barbie maker Mattel has created a doll of the scientist who designed the ill-fated, dangerous Oxford-AZ coronavirus vaccine, Prof. Sarah Gilbert. She was appointed Dame for ‘services to science and to public health in COVID-19 vaccine development’.
1.5 million MHRA-reported adverse reactions and 2200+ UK deaths later, Rishi Sunak continues to prioritise himself. To steal himself an advantage for the top job, he is doing the noble thing 30 months too late. He says he didn’t agree entirely with lockdown, and the SAGE minutes were doctored. Having shanked one Caesar, he is posturing for the next potential one. He cheerfully broke his own lockdown rules while the minions were being terrorised and tackled to the ground by the police. He can hardly style himself as arch-dissident, now.
Of course, he is not the only coward, but unlike the rest of us, he is a multimillionaire. He could have afforded to be a Barbie Hero. I blame myself, too. What did I do? I wrote. Anonymously. However, I was an early voice. Even one of the PM’s family wanted to speak to me in 2020, but I declined the opportunity of being cancelled. The GMC was already crucifying dissenting doctors, as OFCOM was censoring us. It was guerrilla warfare in the NHS – learning on the job as a proto-dissident how not to be discovered by the thought police, whilst retaining one’s ethical standards of medical practice.
I signed every group medic letter I could to counter the propaganda. There was a certain safety in numbers. Most of my cosignatories were retired, senior medics. I wrote to my MP, the PM, his ministers, journalists, the MHRA, PHE and the RCGP. What the hell are you all doing? I asked, Stand up for, safety, the data, and ethics. Either they did not reply, or they hid behind Whitty and his SAGE advice.
On one cold February evening, in 2022 the boiler blew. Boilerman came to the rescue. Not before relieving me of £600 pounds for two hours work plus parts. I ruefully inquired about the prospect of retraining to join him. He was on better money than me. He wholeheartedly encouraged me. He asked what I did:
Doctor.
What’s wrong with that, Bro? he piped.
Going to get sacked. I refused the covid jabs. Getting ready to relocate to Wales or Scotland.
Don’t do that, Bro! I’ve been everywhere, I’m not jabbed. You can buy negative covid tests and vaccine passports! He began to punch out a phone number, answered by some computer geek who sounded like a teenager.
Bro! screamed the plumber, How much for the jabs?
£400 for numbers one and two.
What about the booster, Bro?
£350, Bro.
The plumber protested, why £350?! (For, surely it had to be £400 divided by two?)
Going rate, Bro.
I explained that I could not possibly be dishonest on point of principle. The GMC does not relentlessly hound plumbers out of house and home. He didn’t get it. But wasn’t that what the government wanted? For us to play the game? As long as we were lulled in to an acceptance of biopharmaceutical state terror, digital ID and a centralised digital currency, in principle, what did the government care?
I suspect that significant swathes of the population are jabbed in digital kind only. I know of medical and nursing colleagues who have compacted with each other to achieve the same.
I, like much of the sentient population, am traumatised. Being bombarded constantly by the state for three years into a belief that one’s medical training of 30 years no longer works and no longer matters is psychologically very disorientating. Particularly, like me, if one fought it. I lived in a terror. Terror from the State, from colleagues, from my appraiser and some patients. Terrified of my community and their vaccine interest groups. Terrified of becoming ill and being interned in some covid-deranged, algorithmic NHS hospital. Terrified my family and my children would succumb to coercion to poison. None of them did. They are lucky. I am grateful. Perhaps they might have, but for some facets of the phoney pandemic narrative being rapidly countered by a brave few. Some aspects are unraveling more. Notably, now from the very top, if Sunak’s, Fauci’s and Shapp’s derrière-covering manoeuvres are indicative.
No-one in any position of leadership is yet talking about the worst aspects of this most coordinated and sustained criminal act in history: fabricating the statistics, preventing independent medical practice, and locking us up until their poison was ready. Turning a blind eye to vaccine death and injury, censoring professional concerns, and coercing the population to experimental injection.
Dr Whitty could have and should have just said, no, not on my watch. It was easy. There was no justification for any of it. It was wrong, it was dangerous, it was unnecessary. However, he said yes, and with aplomb. His power in government is illustrated by Bob Moran.
By rubber-stamping and promulgating the government’s covid policies, hasn’t Whitty brought the standards and conduct of our medical profession into disrepute, and damaged its public confidence? Has he protected, promoted and maintained the health, safety and well-being of the public? Where is the GMC to regulate and discipline him? Does it merely enable his professional misconduct? His entire government is so bad it should be charged with corporate manslaughter.
First do no harm. He ought to know the medical fundamental. After all, if not Hippocrates, he is the Chief Medical Officer of England and the Chief Medical Advisor to the UK government. He is supposed to be the highest doctor in the land. Yet, he failed in the basics. He did not need to be a doctor to know as much. A child knows as much.
The lack of safety data and the presence of early danger signals in the initial jab studies, the low mortality from SARS-CoV-2 and the absence of a basis for lockdown and other non-pharmaceutical measures were present from the inception of, quite probably, the worst iatrogenic health disaster in history. Only, Whitty seems uncommonly blind to it all. Whitty did not act in the best interests of anyone or everyone, but perhaps only in his own immediate interests. Whitty should resign.
What is even worse, now the pandemic panic has abated, and the wraps are coming off Pfizer’s self-censored, closely-guarded contrary research, the data (including the ONS’s own) is revealing the very damning scale and pattern of excess mortality following lockdown and each roll out of jabs. The JCVI, MHRA, NHSE and government continue to come for us and our children, with dual-strain concoctions of what already is demonstrably unnecessary, dangerous and ineffective. The new, alleged omicron-targeting versions are not tested in humans and compound the rushed, unsafe MHRA, CDC and FDA practices of previous covid jab approvals.
What is Whitty and his government thinking? If Whitty realises he may about to be fingered, how does he live with himself? He has limited exit strategies. He is 56. It is unrealistic for him to take the wrong knee at the Chelsea-Fulham derby and then announce a glorious, postponed Fauci-esque retirement.
Dame Dr. June Raine, Chief Executive, Medicines and Healthcare products Enabling Agency. She was appointed Dame ‘for services to Healthcare and the Covid-19 Response’.
Another culpable, leading doctor is Dr June Raine, Chief Executive of the MHRA. She doesn’t think so, at all. Furthermore, she says she no longer believes she is a regulator. It certainly appears she is not able to be regulated. In March 2022, she was filmed, with no sign on contrition, giving a talk at her alma mater. I found it chilling and unreal. She came across as a converted pharmaceutical spokesperson not working primarily for public safety. She acted as if she were a master in command of all facts covid. She used the terms, ‘build back better’, ‘tearing up the rule book’ and ‘layers of parallel working’ (rushing) ‘that can never be turned back’.
The name of her talk?From Watchdog to Enabler. This is concerning. The R is for Regulation. If it is changed from that to E, one gets MHEA, Medicines and Healthcare products Enabling Agency. Even more concerning because she has been enabling a MHRA principal funder, Bill Gates, to make billions more from his wonderful vaccines by blindsiding her own damning MHRA injury and death statistics. What is she thinking? Why isn’t she doing something to regulate the madness? Dr Raine was appointed Dame ‘for services to Healthcare and the Covid-19 Response’.
Incidentally, the NHS is on fxxxxxgfire. I said so to my practice manager. She readily agreed. Never has it been so bad. It is razing itself to the ground in the heat of its own lies, aggression and failures. A staff united around basic medical ethics could have easily extinguished the flames, but no one seemed to care.
One work colleague particular intrigues me. Like others, he continues to choose to prowl around the practice like a startled meerkat with a perma-mask. I haven’t seen his face for months. It was already baffling, but became even more so. His face-to-face patient was diverted to me by the receptionist. The reason given on the computerised appointment was ‘not vaccinated’. It was confusing. Who was not vaccinated? My colleague, me, or the patient? And, so what? In the fog of NHS time pressures, I did not have time to conduct an investigation. It would also have invited an uncomfortable conversation about my own, unknown un-injected status. The diversion begged a question. Had my meerkat colleague declined to see a patient because he was not, or his patient was not injected?
The patients know the crack. Most are done with masks and serial jabs. They are too polite to say so, unless invited to. When invited, they do not hold back. The baby boomers know the taxes they paid for healthcare from cradle to grave have been squandered. Everything NHS is rendered telephonic and spastic by covid. Designed to pretend to be delivering healthcare. The public are no longer fooled. Just as they resigned themselves to being lab rats, they have resigned themselves to undiagnosed and untreated cancers. There has been a palpable increased prevalence or incidence of cancers in my practice. It is reasonable to suspect this is due to misguided covid policy, and as research suggests, the covid jabs. Skin and bladder cancers seem very prominent where I am. The dermatology service have given up even pretending photographs can diagnose cancer within the gold standard two weeks. The reply now is, we’re sorry we simply cannot see your patient for at least 6 months.
From reading a patient’s notes it can all look so meticulously documented and competent, with regular appointments, contacts and consultations. But the in vivo, rotting patient tells the real story, once he or she manages to get an appointment face-to-face. They have actually not been seen for over two years. Everything, from physiotherapy, cardiology, general practice and reviews of longterm conditions has been over the phone, or ‘telephonic’ as some of my colleagues formalise this most negligent of practices. Home visits are the most time-consuming consultations. The current capacity, resources and will for this are nearly zero. Visits to the most vulnerable at home are severely rationed beyond the point of danger. It is always shocking to me. It is the wrong way round. Only the fittest, least vulnerable, and most assertive in our transformed Hunger GamesNHS possess the prowess to physically cross the threshold to meet a doctor. It is such a lowly standard of medical practice. Certifying the dead by video call is a new inhuman low for NHS Digital.
Where does that leave patients? To fester or to private practice. This is exactly how it is going.
It is most distressing to deal with ever-poorer patients who have been led to believe the NHS has healthcare that it no longer can afford or deliver. It is even worse when someone who is malnourished and cannot afford adequate clothing asks for a letter of private referral for basic radiological investigations. Wouldn’t it be best to admit failure so patients can either make other arrangements or otherwise organise a rebellion?
When thinking of Fauci and Whitty I cannot help but think of Dr Harold Shipman. Aside from history’s tyrants, Shipman is one of the modern world’s most prolific serial killers. The other two doctors are, arguably, measurably worse in the harm each has caused to their country’s health and mortality rates. The data is becoming more damning. On the evidence it can be construed that there was no exceptionally fatal respiratory viral infection pandemic, and further, not only a test-demic but also widely injurious and fatal lockdown and vaccine-induced pandemics. This recent German paper encompasses most of it, and is summarised by eugyppius.
The staff attrition rate in general practice is astonishing. Illness, sabbaticals, resignation, nervous breakdown, retraining, lay-off, it is all happening. GP medical partners are jumping ship and selling out to private enterprise. They cannot bear it. Is some element of the exodus professional guilt? A nagging consciousness of the degradation within their professional souls? I hope so. One cannot hold a rictus smile, forever. Covid has been the final nail. Very soon, general practice will fall the same way as NHS dentists in the 1990s. There will be none. The cancerous will join the edentulous on the streets. In one, already-failing practice pretending to offer care via handset and batteries of remote, platitudinal investigations (instigated by covid policy), 4 out of 10 doctors were laid off, including me. How, I asked, would they deliver proper healthcare? The manager’s reply was ironic. The (company-owned) practice could not afford to offset the recent 1.25% National Insurance levy without cutting staff. This is Sunak’s extra tax to revive the NHS after he first exsanguinated it under guise of covid. He has zombified it.
The boomers know they cannot expect timely nor safe healthcare, anymore. But they are gracious and grateful, We’ve been lucky until now. They are right, they were the golden billion. They rode the crest of the post-imperial wave. What about you younger ones? It is not just the want of health and jobs for them, it is soon to be the want of the basic means to survive.
I will never implicitly trust a pharmaceutical product, drug company, royal college, medical journal or the State again. Not least vaccines or the NHS. This is how it has to be. It is not ideal when one is a NHS doctor. This is the damage wanton greed and a total disregard of people creates.
The profession’s complicit silence is killing its own young doctors: their death rate is 23 times more post-second jab in Canada, a country rabid for toxin mandates. The profession cannot even protect its own, having transformed into lame ducks and lemmings (as well as masked meerkats) at the click of a tyrant’s fingers.
Do not believe the tyranny is over. It has only just begun. There is no room for complacency.
1st September 2022
All links are archived and if broken may, in the majority, be found by searching the link on archive.is or, in the small minority, onweb.archive.org
The Covid Physician is (still) an unheroic NHS doctor. This article is a personal view and does not necessarily represent the views of the NHS. Patient details have been anonymised.